Evaluation of the Efficacy of Doxycycline, Ciprofloxacin, Levofloxacin, and Co-trimoxazole Using In Vitro and In Vivo Models of Q Fever
- PMID: 34370577
- PMCID: PMC8522727
- DOI: 10.1128/AAC.00673-21
Evaluation of the Efficacy of Doxycycline, Ciprofloxacin, Levofloxacin, and Co-trimoxazole Using In Vitro and In Vivo Models of Q Fever
Abstract
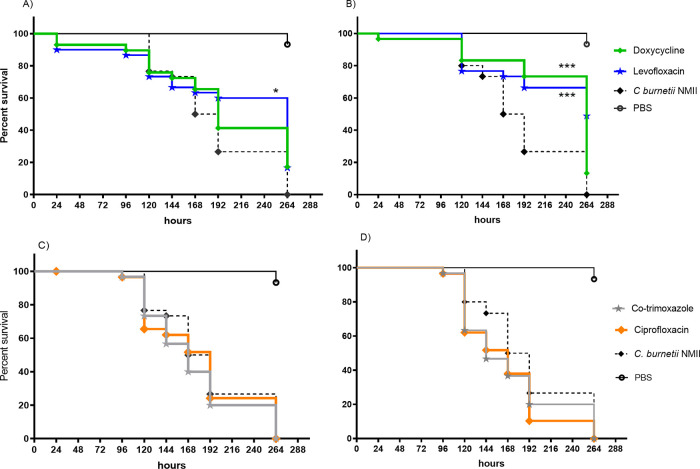
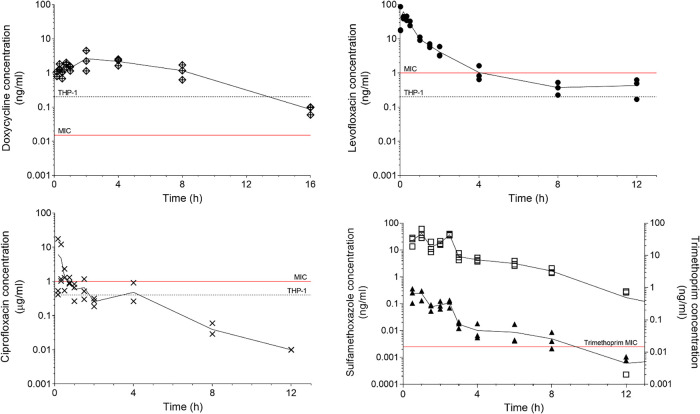
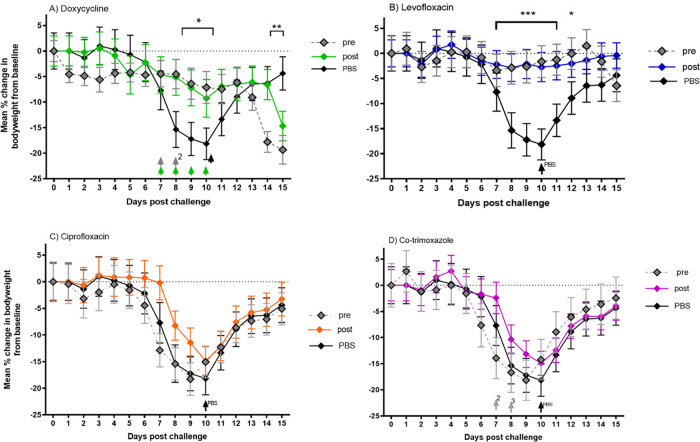
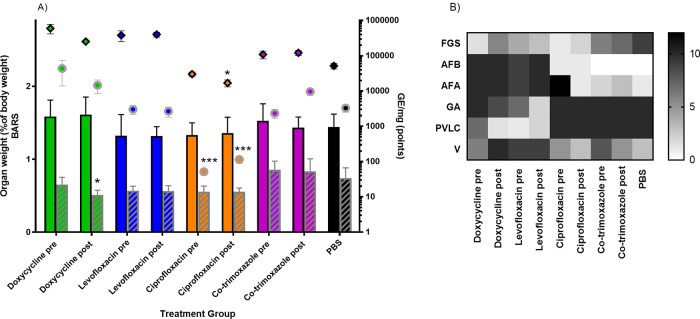
Q fever, caused by the intracellular pathogen Coxiella burnetii, is traditionally treated using tetracycline antibiotics, such as doxycycline. Doxycycline is often poorly tolerated, and antibiotic-resistant strains have been isolated. In this study, we have evaluated a panel of antibiotics (doxycycline, ciprofloxacin, levofloxacin, and co-trimoxazole) against C. burnetii using in vitro methods (determination of MIC using liquid and solid media; efficacy assessment in a THP cell infection model) and in vivo methods (wax moth larvae and mouse models of infection). In addition, the schedule for antibiotic treatment has been evaluated, with therapy initiated at 24 h pre- or postchallenge. Both doxycycline and levofloxacin limited overt clinical signs during treatment in the AJ mouse model of aerosol infection, but further studies are required to investigate the possibility of disease relapse or incomplete bacterial clearance after the antibiotics are stopped. Levofloxacin was well tolerated and therefore warrants further investigation as an alternative to the current recommended treatment with doxycycline.
Keywords: Coxiella; Q fever; antibiotic; treatment.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- van der Hoek W, Hogema BM, Dijkstra F, Rietveld A, Wijkmans CJ, Schneeberger PM, Zaaijer HL. 2012. Relation between Q fever notifications and Coxiella burnetii infections during the 2009 outbreak in The Netherlands. Euro Surveill 17:20058. - PubMed
-
- Limonard GJ, Nabuurs-Franssen MH, Weers-Pothoff G, Wijkmans C, Besselink R, Horrevorts AM, Schneeberger PM, Groot CA. 2010. One-year follow-up of patients of the ongoing Dutch Q fever outbreak: clinical, serological and echocardiographic findings. Infection 38:471–477. 10.1007/s15010-010-0052-x. - DOI - PMC - PubMed
-
- Kampschreur LM, Delsing CE, Groenwold RH, Wegdam-Blans MC, Bleeker-Rovers CP, de Jager-Leclercq MG, Hoepelman AI, van Kasteren ME, Buijs J, Renders NH, Nabuurs-Franssen MH, Oosterheert JJ, Wever PC. 2014. Chronic Q fever in the Netherlands 5 years after the start of the Q fever epidemic: results from the Dutch chronic Q fever database. J Clin Microbiol 52:1637–1643. 10.1128/JCM.03221-13. - DOI - PMC - PubMed
-
- Pebody RG, Wall PG, Ryan MJ, Fairley C. 1996. Epidemiological features of Coxiella burnetii infection in England and Wales: 1984 to 1994. Commun Dis Rep CDR Rev 6:R128–32. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources