Gender disparity in cases enrolled in clinical trials of visceral leishmaniasis: A systematic review and meta-analysis
- PMID: 33725005
- PMCID: PMC7963105
- DOI: 10.1371/journal.pntd.0009204
Gender disparity in cases enrolled in clinical trials of visceral leishmaniasis: A systematic review and meta-analysis
Abstract
Background: A higher caseload of visceral leishmaniasis (VL) has been observed among males in community-based surveys. We carried out this review to investigate how the observed disparity in gender distribution is reflected in clinical trials of antileishmanial therapies.
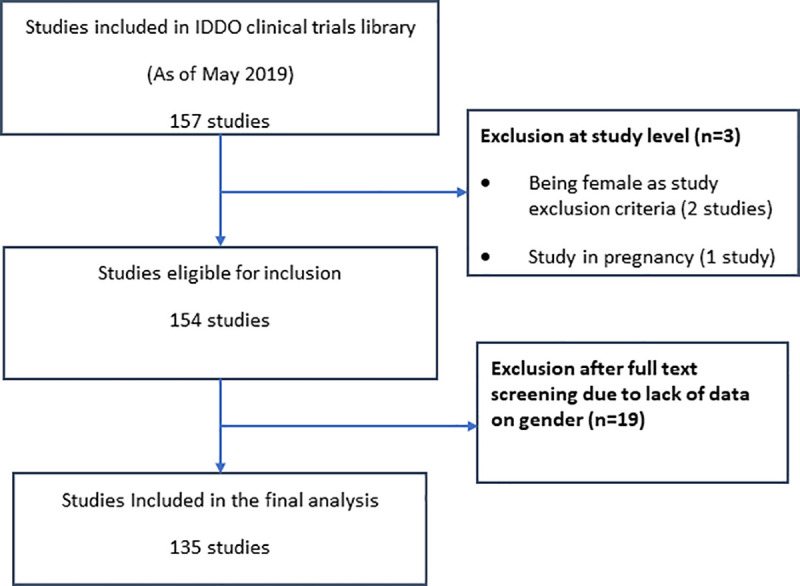
Methods: We identified relevant studies by searching a database of all published clinical trials in VL from 1980 through 2019 indexed in the Infectious Diseases Data Observatory (IDDO) VL clinical trials library. The proportion of male participants enrolled in studies eligible for inclusion in this review were extracted and combined using random effects meta-analysis of proportion. Results were expressed as percentages and presented with respective 95% confidence intervals (95% CIs). Heterogeneity was quantified using I2 statistics and sub-group meta-analyses were carried out to explore the sources of heterogeneity.
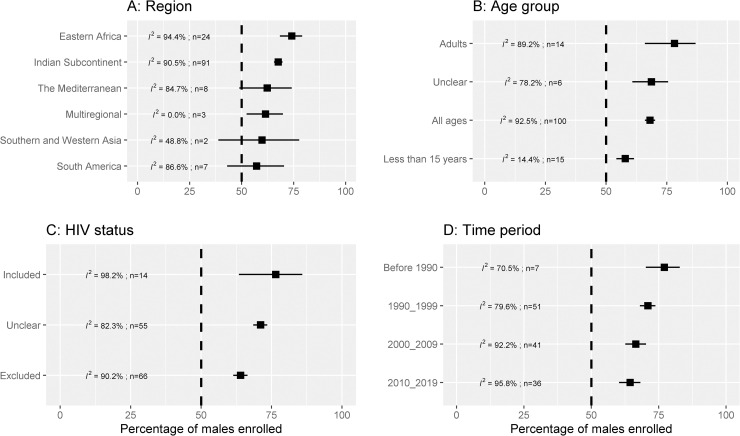
Results: We identified 135 published studies (1980-2019; 32,177 patients) with 68.0% [95% CI: 65.9%-70.0%; I2 = 92.6%] of the enrolled participants being males. The corresponding estimates were 67.6% [95% CI: 65.5%-69.7%; n = 91 trials; I2 = 90.5%; 24,218 patients] in studies conducted in the Indian sub-continent and 74.1% [95% CI: 68.4%-79.1%; n = 24 trials; I2 = 94.4%; 6,716 patients] in studies from Eastern Africa. The proportion of male participants was 57.9% [95% CI: 54.2%-61.5%] in studies enrolling children aged <15 years, 78.2% [95% CI: 66.0%-86.9%] in studies that enrolled adults (≥15 years), and 68.1% [95% CI: 65.9%-70.0%] in studies that enrolled patients of all ages. There was a trend for decreased proportions of males enrolled over time: 77.1% [95% CI: 70.2%-82.8%; 1356 patients] in studies published prior to the 1990s whereas 64.3% [95% CI: 60.3%-68.2%; 15,611 patients] in studies published on or after 2010. In studies that allowed the inclusion of patients with HIV co-infections, 76.5% [95% CI: 63.8%-85.9%; 5,123 patients] were males and the corresponding estimate was 64.0% [95% CI: 61.4%-66.5% 17,500 patients] in studies which excluded patients with HIV co-infections.
Conclusions: Two-thirds of the participants enrolled in clinical studies in VL conducted in the past 40 years were males, though the imbalance was less in children and in more recent trials. VL treatment guidelines are informed by the knowledge of treatment outcomes from a population that is heavily skewed towards adult males. Investigators planning future studies should consider this fact and ensure approaches for more gender-balanced inclusion.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Rogers SL. Report of an investigation of the epidemic of malarial fever in Assam or Kala-Azar. Shillong, Assam: Assam Secretariat Printing Office; 1897.
-
- Rogers SL. Kala-Azar. Fever Trop. Third Edit. London: Henry Frowde and Hodder and Stoughton; 1919. p. 21.
-
- Brahmachari U. A treatise on Kala-Azar. London: John Bale, Sons & Danielsson Ltd; 1928.
-
- Archibald RG. Some observations on the epidemiology of kala-azar in the sudan. Trans. R. Soc. Trop. Med. Hyg. 1937;XXX:395–406.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous