Effectiveness of a sepsis programme in a resource-limited setting: a retrospective analysis of data of a prospective observational study (Ubon-sepsis)
- PMID: 33602702
- PMCID: PMC7896572
- DOI: 10.1136/bmjopen-2020-041022
Effectiveness of a sepsis programme in a resource-limited setting: a retrospective analysis of data of a prospective observational study (Ubon-sepsis)
Abstract
Objective: To evaluate the effectiveness of a Sepsis Fast Track (SFT) programme initiated at a regional referral hospital in Thailand in January 2015.
Design: A retrospective analysis using the data of a prospective observational study (Ubon-sepsis) from March 2013 to January 2017.
Setting: General medical wards and medical intensive care units (ICUs) of a study hospital.
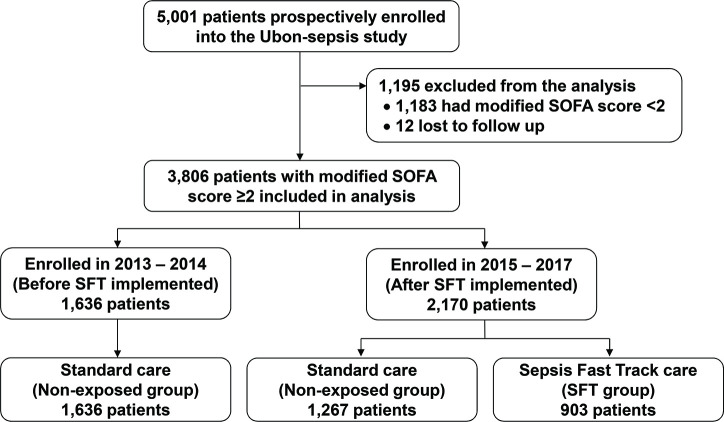
Participants: Patients with community-acquired sepsis observed under the Ubon-sepsis cohort. Sepsis was defined as modified Sequential Organ Failure Assessment (SOFA) Score ≥2.
Main exposure: The SFT programme was a protocol to identify and initiate sepsis care on hospital admission, implemented at the study hospital in 2015. Patients in the SFT programme were admitted directly to the ICUs when available. The non-exposed group comprised of patients who received standard of care.
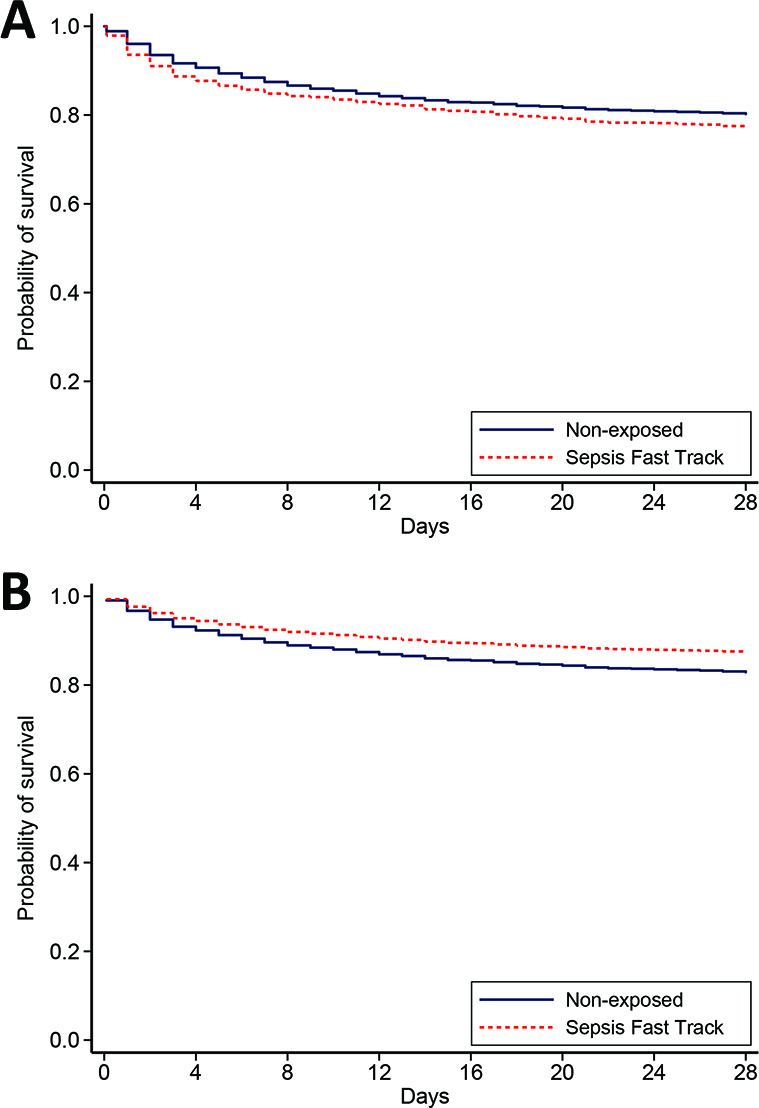
Main outcome: The primary outcome was 28-day mortality. The secondary outcomes were measured sepsis management interventions.
Results: Of 3806 sepsis patients, 903 (24%) were detected and enrolled in the SFT programme of the study hospital (SFT group) and 2903 received standard of care (non-exposed group). Patients in the SFT group had more organ dysfunction, were more likely to receive measured sepsis management and to be admitted directly to the ICU (19% vs 4%). Patients in the SFT group were more likely to survive (adjusted HR 0.72, 95% CI 0.58 to 0.88, p=0.001) adjusted for admission year, gender, age, comorbidities, modified SOFA Score and direct admission to the ICUs.
Conclusions: The SFT programme is associated with improved sepsis care and lower risk of death in sepsis patients in rural Thailand, where some critical care resources are limited. The survival benefit is observed even when all patients enrolled in the programme could not be admitted directly into the ICUs.
Trial registration number: NCT02217592.
Keywords: epidemiology; infectious diseases; intensive & critical care.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
{kind=link}
{kind=link}
References
-
- WHO WHO sepsis technical expert meeting - meeting report Geneva: World Health Organization, 2018. Available: https://www.who.int/servicedeliverysafety/areas/sepsis_meeting-report-20... [Accessed 25 Nov 2019].
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical