Population-Based Prevalence of Chlamydia trachomatis Infection and Antibodies in Four Districts with Varying Levels of Trachoma Endemicity in Amhara, Ethiopia
- PMID: 33200728
- PMCID: PMC7790060
- DOI: 10.4269/ajtmh.20-0777
Population-Based Prevalence of Chlamydia trachomatis Infection and Antibodies in Four Districts with Varying Levels of Trachoma Endemicity in Amhara, Ethiopia
Abstract
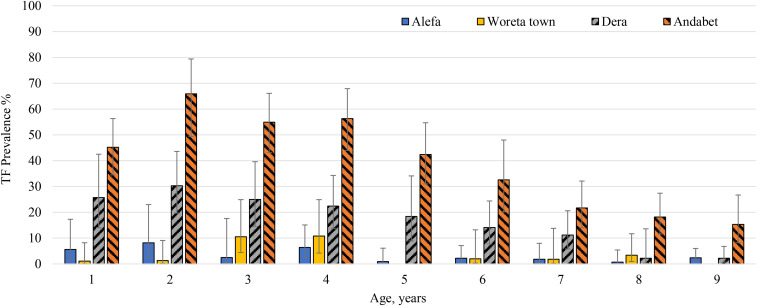
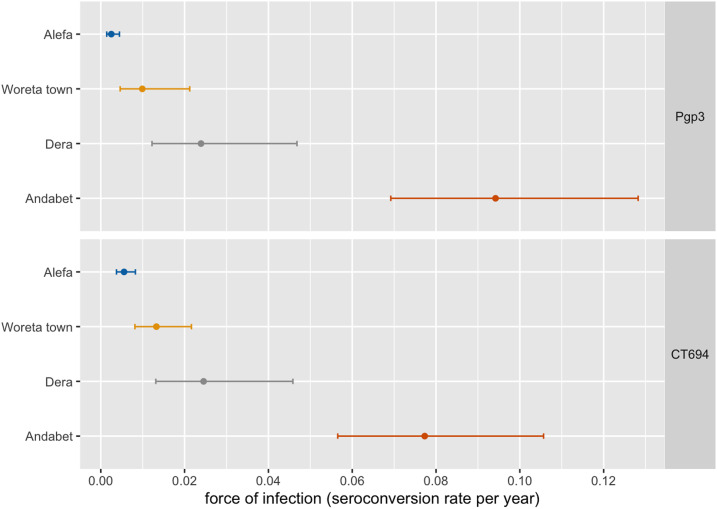
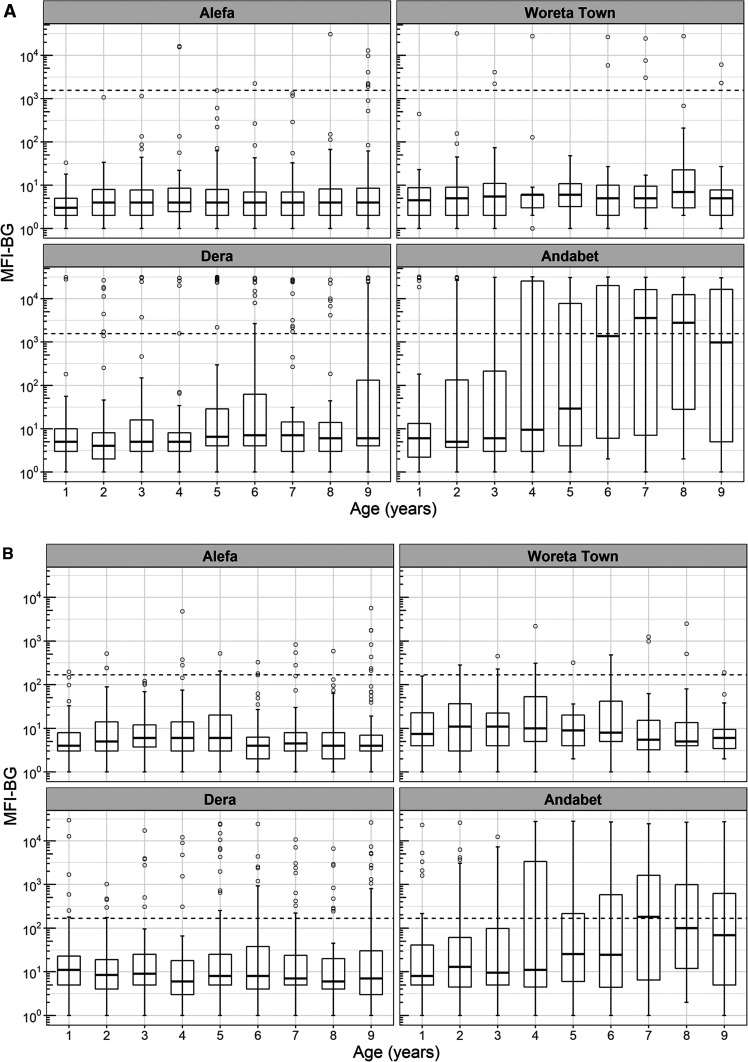
The Trachoma Control Program in Amhara region, Ethiopia, scaled up the surgery, antibiotics, facial cleanliness, and environmental improvement (SAFE) strategy in all districts starting in 2007. Despite these efforts, many districts still require additional years of SAFE. In 2017, four districts were selected for the assessment of antibody responses against Chlamydia trachomatis antigens and C. trachomatis infection to better understand transmission. Districts with differing endemicity were chosen, whereby one had a previous trachomatous inflammation-follicular (TF) prevalence of ≥ 30% (Andabet), one had a prevalence between 10% and 29.9% (Dera), one had a prevalence between 5% and 10% (Woreta town), and one had a previous TF prevalence of < 5% (Alefa) and had not received antibiotic intervention for 2 years. Survey teams assessed trachoma clinical signs and took conjunctival swabs and dried blood spots (DBS) to measure infection and antibody responses. Trachomatous inflammation-follicular prevalence among children aged 1-9 years was 37.0% (95% CI: 31.1-43.3) for Andabet, 14.7% (95% CI: 10.0-20.5) for Dera, and < 5% for Woreta town and Alefa. Chlamydia trachomatis infection was only detected in Andabet (11.3%). Within these districts, 2,195 children provided DBS. The prevalence of antibody responses to the antigen Pgp3 was 36.9% (95% CI: 29.0-45.6%) for Andabet, 11.3% (95% CI: 5.9-20.6%) for Dera, and < 5% for Woreta town and Alefa. Seroconversion rate for Pgp3 in Andabet was 0.094 (95% CI: 0.069-0.128) events per year. In Andabet district, where SAFE implementation has occurred for 11 years, the antibody data support the finding of persistently high levels of trachoma transmission.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous