Estimating unobserved SARS-CoV-2 infections in the United States
- PMID: 32826332
- PMCID: PMC7486725
- DOI: 10.1073/pnas.2005476117
Estimating unobserved SARS-CoV-2 infections in the United States
Abstract
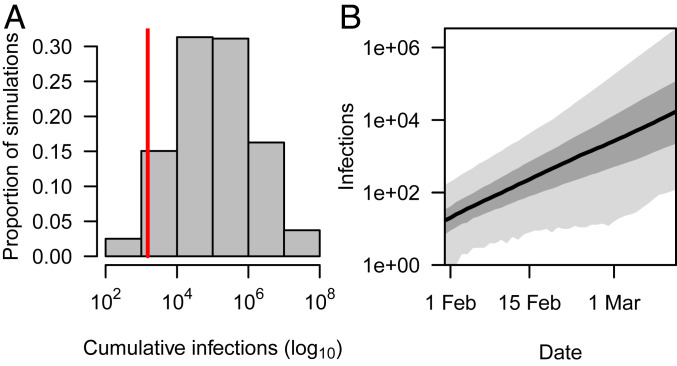
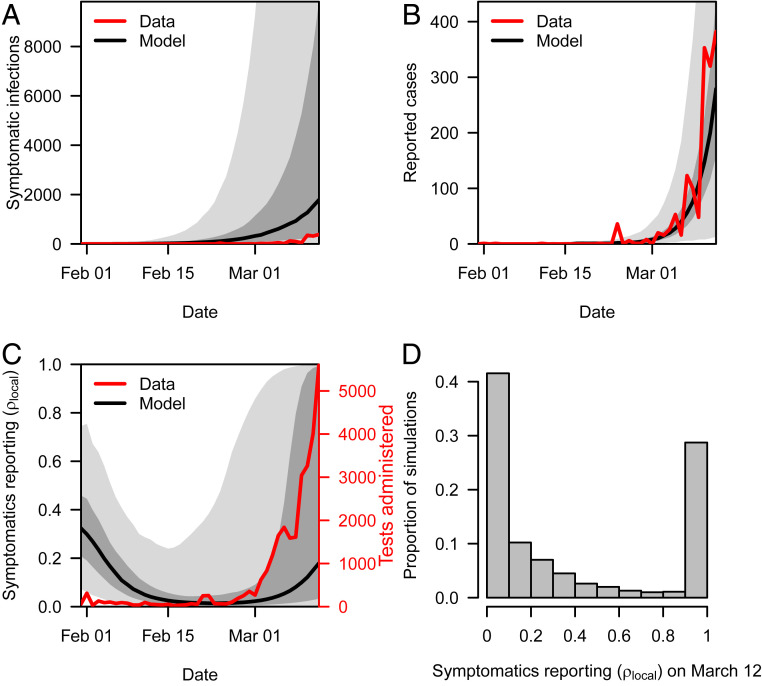
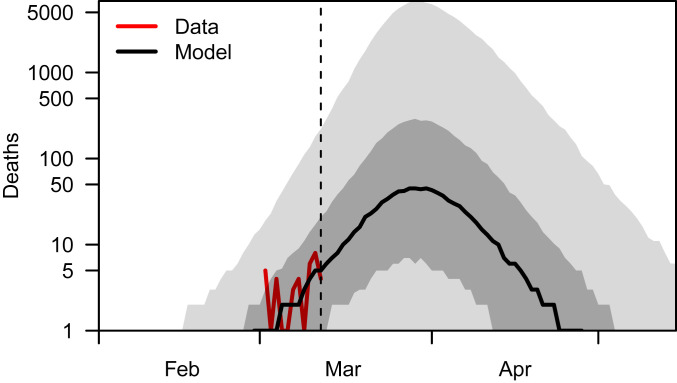
By March 2020, COVID-19 led to thousands of deaths and disrupted economic activity worldwide. As a result of narrow case definitions and limited capacity for testing, the number of unobserved severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections during its initial invasion of the United States remains unknown. We developed an approach for estimating the number of unobserved infections based on data that are commonly available shortly after the emergence of a new infectious disease. The logic of our approach is, in essence, that there are bounds on the amount of exponential growth of new infections that can occur during the first few weeks after imported cases start appearing. Applying that logic to data on imported cases and local deaths in the United States through 12 March, we estimated that 108,689 (95% posterior predictive interval [95% PPI]: 1,023 to 14,182,310) infections occurred in the United States by this date. By comparing the model's predictions of symptomatic infections with local cases reported over time, we obtained daily estimates of the proportion of symptomatic infections detected by surveillance. This revealed that detection of symptomatic infections decreased throughout February as exponential growth of infections outpaced increases in testing. Between 24 February and 12 March, we estimated an increase in detection of symptomatic infections, which was strongly correlated (median: 0.98; 95% PPI: 0.66 to 0.98) with increases in testing. These results suggest that testing was a major limiting factor in assessing the extent of SARS-CoV-2 transmission during its initial invasion of the United States.
Keywords: coronavirus; emerging infectious disease; mathematical modeling; public health surveillance; silent transmission.
Copyright © 2020 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- World Health Organization , Geneva, Switzerland. "Coronavirus disease 2019 (COVID-19) situation report" (Tech. Rep. 51, 2020).
-
- van Doremalen N., et al. , Aerosol and surface stability of HCoV-19 (SARS-CoV-2) compared to SARS-CoV-1. medRxiv:2020年03月09日.20033217 (13 March 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous