Impact of Different Mass Drug Administration Strategies for Gaining and Sustaining Control of Schistosoma mansoni and Schistosoma haematobium Infection in Africa
- PMID: 32400356
- PMCID: PMC7351298
- DOI: 10.4269/ajtmh.19-0829
Impact of Different Mass Drug Administration Strategies for Gaining and Sustaining Control of Schistosoma mansoni and Schistosoma haematobium Infection in Africa
Abstract
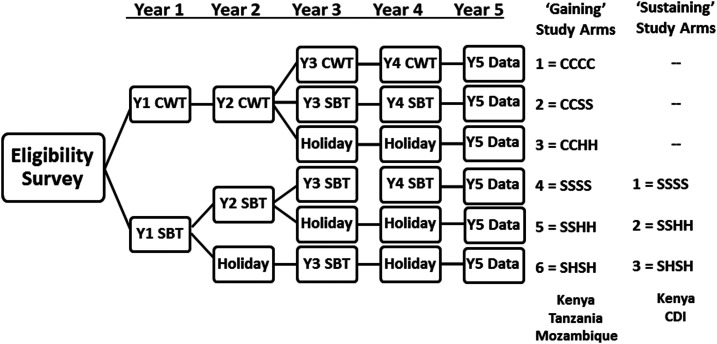
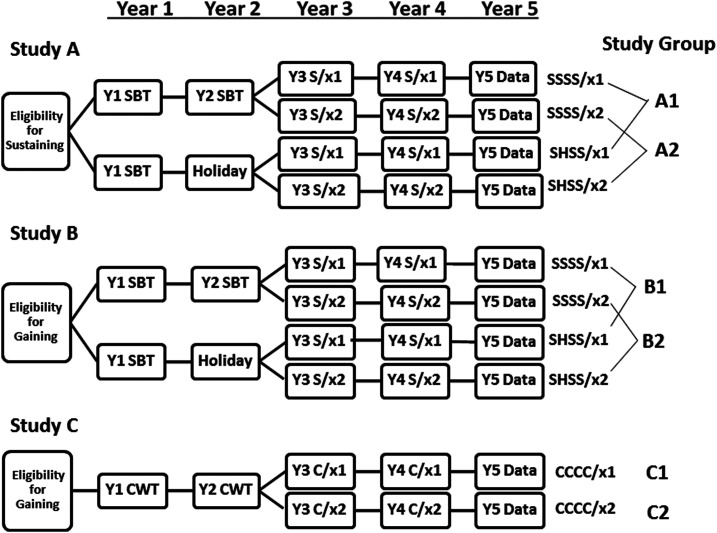
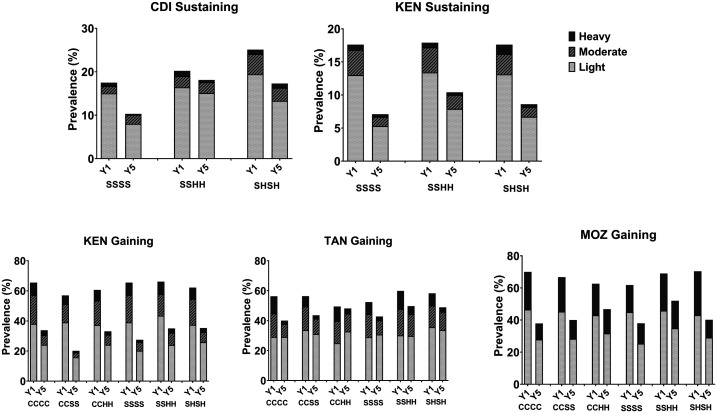
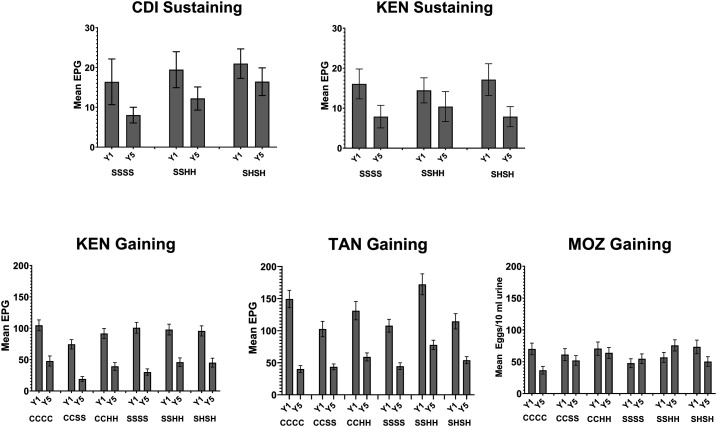
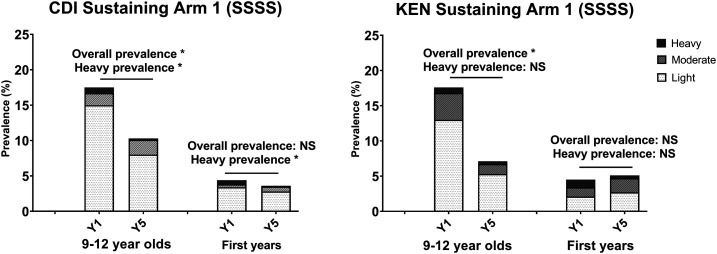
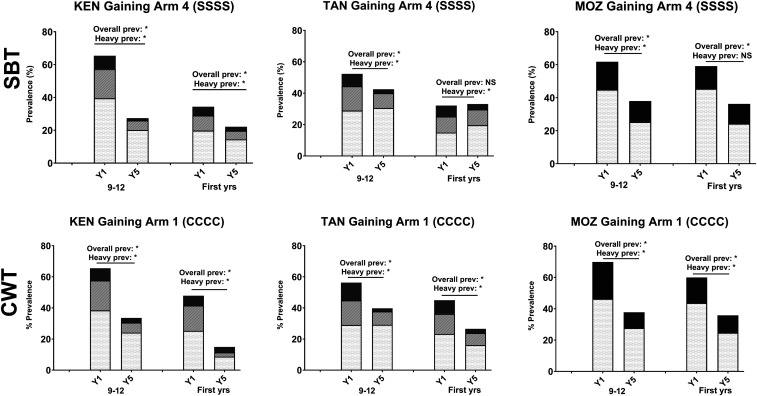
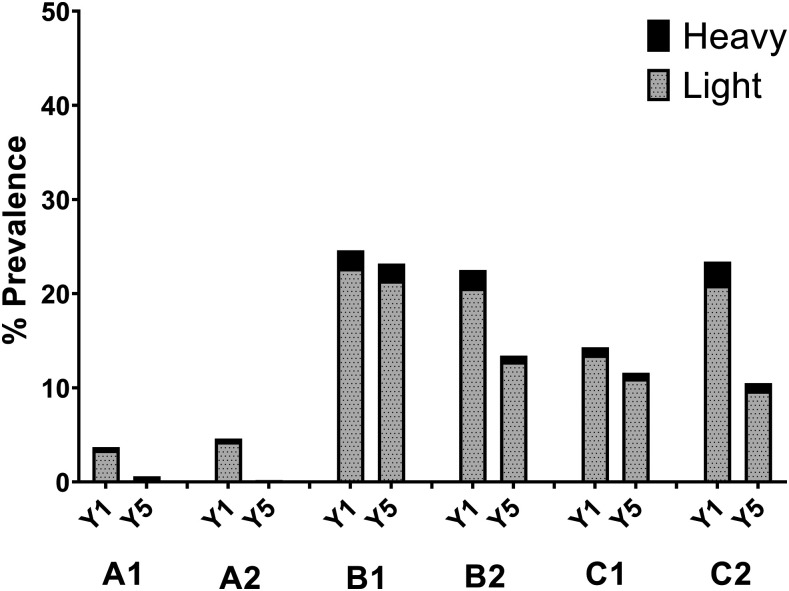
This report summarizes the design and outcomes of randomized controlled operational research trials performed by the Bill & Melinda Gates Foundation-funded Schistosomiasis Consortium for Operational Research and Evaluation (SCORE) from 2009 to 2019. Their goal was to define the effectiveness and test the limitations of current WHO-recommended schistosomiasis control protocols by performing large-scale pragmatic trials to compare the impact of different schedules and coverage regimens of praziquantel mass drug administration (MDA). Although there were limitations to study designs and performance, analysis of their primary outcomes confirmed that all tested regimens of praziquantel MDA significantly reduced local Schistosoma infection prevalence and intensity among school-age children. Secondary analysis suggested that outcomes in locations receiving four annual rounds of MDA were better than those in communities that had treatment holiday years, in which no praziquantel MDA was given. Statistical significance of differences was obscured by a wider-than-expected variation in community-level responses to MDA, defining a persistent hot spot obstacle to MDA success. No MDA schedule led to elimination of infection, even in those communities that started at low prevalence of infection, and it is likely that programs aiming for elimination of transmission will need to add supplemental interventions (e.g., snail control, improvement in water, sanitation and hygiene, and behavior change interventions) to achieve that next stage of control. Recommendations for future implementation research, including exploration of the value of earlier program impact assessment combined with intensification of intervention in hot spot locations, are discussed.
Conflict of interest statement
Trials registration: The studies discussed in this article are registered at International Standard Randomised Controlled Trial registry (
Data availability: Data collected in SCORE studies will be housed and made accessible to the global research community through Clinical Epidemiology Database Resources, ClinEpiDB (
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the U.S. Centers for Disease Control and Prevention or of the World Health Organization.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Homeida MM, Eltoum IA, Ali MM, Suliaman SM, Elobied EA, Mansour M, Saad AM, Bennett JL, 1996. The effectiveness of annual versus biennial mass chemotherapy in reducing morbidity due to schistosomiasis: a prospective study in Gezira-Managil, Sudan. Am J Trop Med Hyg 54: 140–145. - PubMed
-
- Garba A, Campagne G, Tassie JM, Barkire A, Vera C, Sellin B, Chippaux JP, 2004. Long-term impact of a mass treatment by praziquantel on morbidity due to Schistosoma haematobium in two hyperendemic villages of Niger [article in French]. Bull Soc Pathol Exot 97: 7–11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials