Mass campaigns combining antimalarial drugs and anti-infective vaccines as seasonal interventions for malaria control, elimination and prevention of resurgence: a modelling study
- PMID: 31664924
- PMCID: PMC6820916
- DOI: 10.1186/s12879-019-4467-4
Mass campaigns combining antimalarial drugs and anti-infective vaccines as seasonal interventions for malaria control, elimination and prevention of resurgence: a modelling study
Abstract
Background: The only licensed malaria vaccine, RTS,S/AS01, has been developed for morbidity-control in young children. The potential impact on transmission of deploying such anti-infective vaccines to wider age ranges, possibly with co-administration of antimalarial treatment, is unknown. Combinations of existing malaria interventions is becoming increasingly important as evidence mounts that progress on reducing malaria incidence is stalling and threatened by resistance.
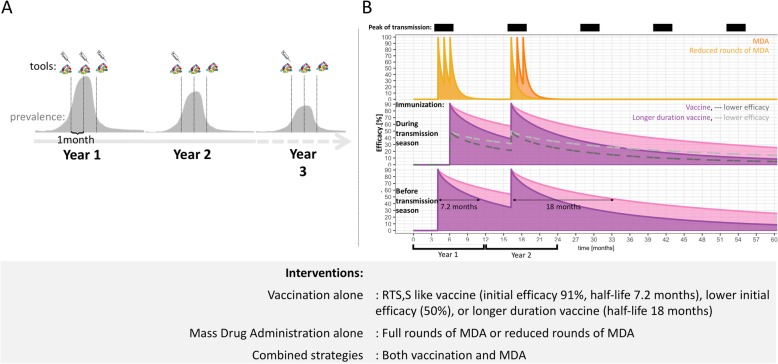
Methods: Malaria transmission and intervention dynamics were simulated using OpenMalaria, an individual-based simulation model of malaria transmission, by considering a seasonal transmission setting and by varying epidemiological and setting parameters such as transmission intensity, case management, intervention types and intervention coverages. Chemopreventive drugs and anti-infective vaccine efficacy profiles were based on previous studies in which model parameters were fitted to clinical trial data. These intervention properties were used to evaluate the potential of seasonal mass applications of preventative anti-infective malaria vaccines, alone or in combination with chemoprevention, to reduce malaria transmission, prevent resurgence, and/or reach transmission interruption.
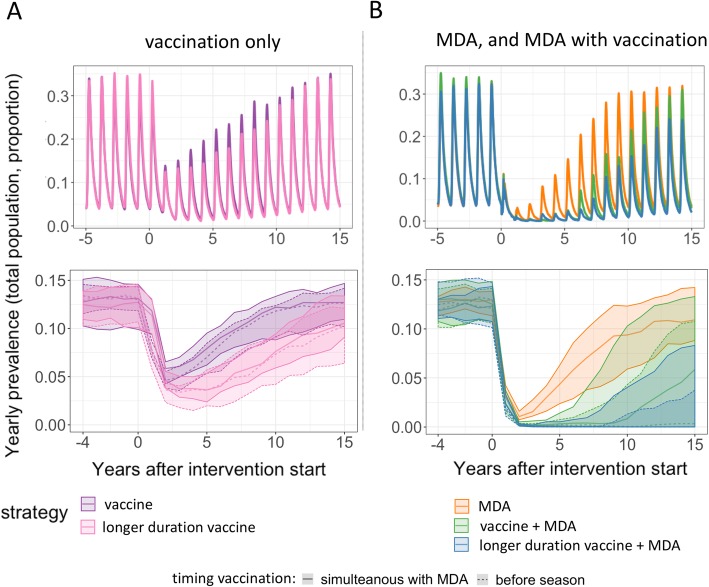
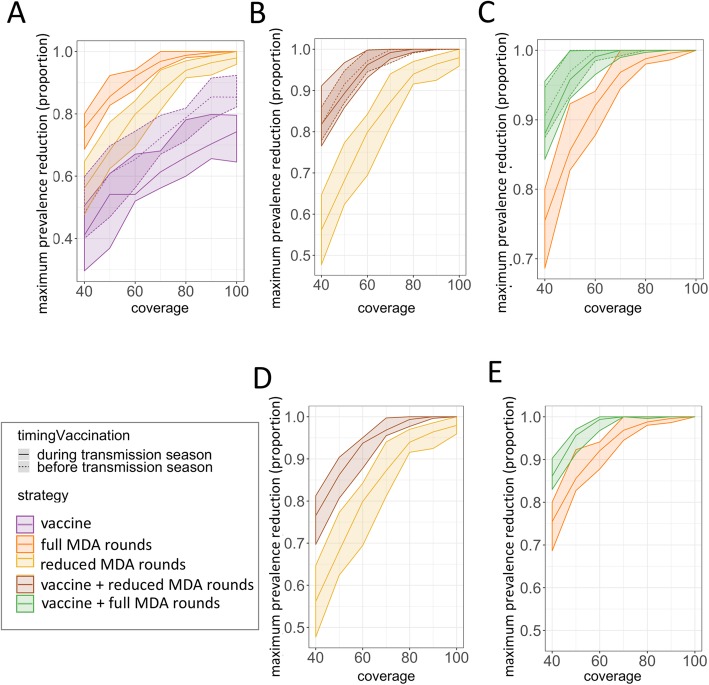
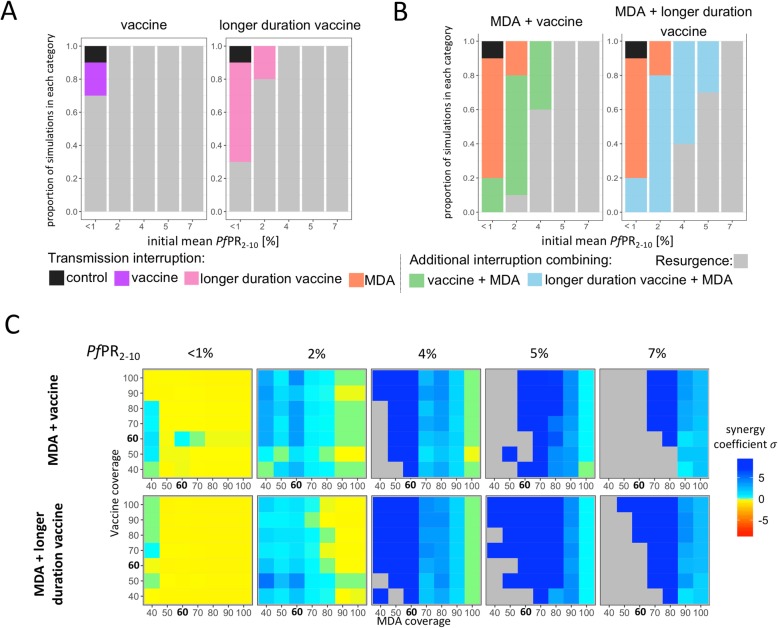
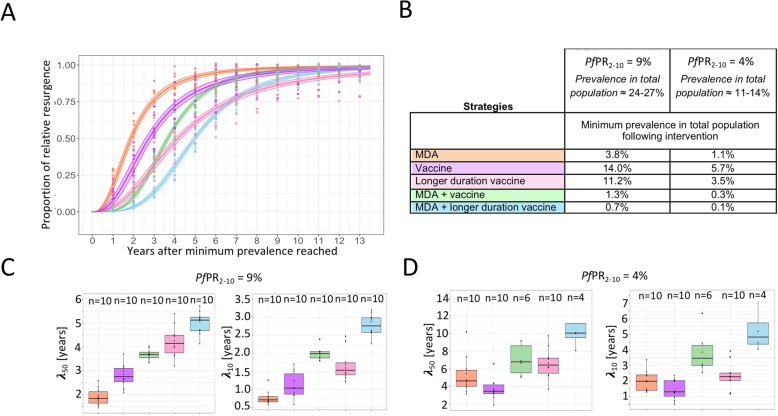
Results: Deploying a vaccine to all ages on its own is a less effective intervention strategy compared to chemoprevention alone. However, vaccines combined with drugs are likely to achieve dramatic prevalence reductions and in few settings, transmission interruption. The combined mass intervention will result in lower prevalence following the intervention compared to chemoprevention alone and will increase chances of interruption of transmission resulting from a synergistic effect between both interventions. The combination of vaccine and drug increases the time before transmission resurges after mass interventions cease compared to mass treatment alone. Deploying vaccines and drugs together requires fewer rounds of mass intervention and fewer years of intervention to achieve the same public health impact as chemoprevention alone.
Conclusions: Through simulations we identified a previously unidentified value of deploying vaccines with drugs, namely the greatest benefit will be in preventing and delaying transmission resurgence for longer periods than with other human targeted interventions. This is suggesting a potential role for deploying vaccines alongside drugs in transmission foci as part of surveillance-response strategies.
Keywords: Malaria; Mass intervention; Resurgence; Seasonal transmission; Simulation; Vaccine.
Conflict of interest statement
CFO and CL are part of the PATH’s Malaria Vaccine Initiative.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- World Health Organization (WHO). Global technical strategy for malaria 2016–2030. WHO Geneva. 2015. 1–35 p.
-
- World Health Organization (WHO). World Malaria Report. 2017:2017.
-
- European Medicines Agency First malaria vaccine receives positive scientific opinion from EMA. Press Release. 2015;44(July):1–3.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources