Exploring the parasite load and molecular diversity of Trypanosoma cruzi in patients with chronic Chagas disease from different regions of Brazil
- PMID: 30418976
- PMCID: PMC6258420
- DOI: 10.1371/journal.pntd.0006939
Exploring the parasite load and molecular diversity of Trypanosoma cruzi in patients with chronic Chagas disease from different regions of Brazil
Abstract
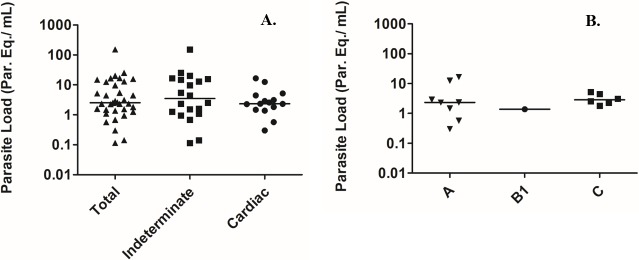
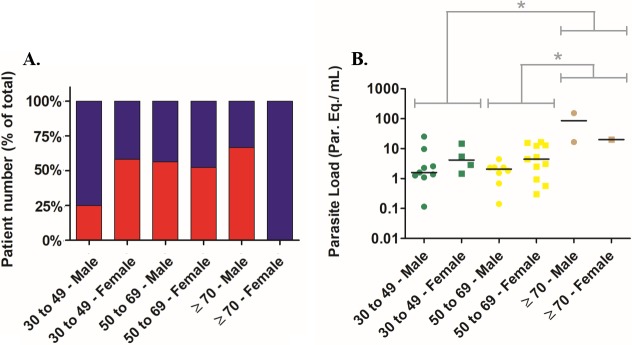
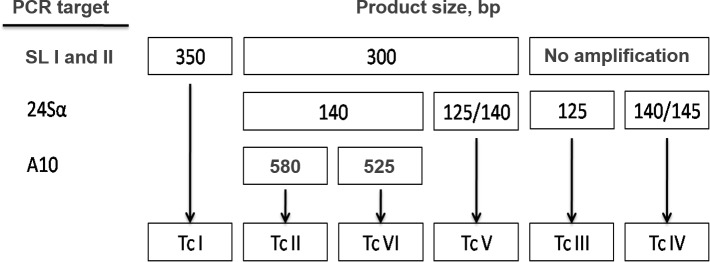
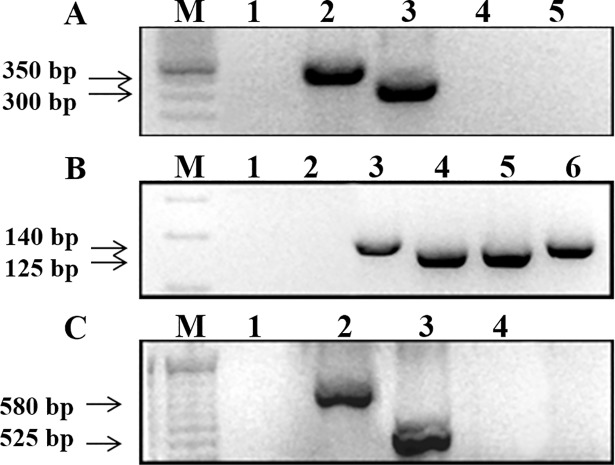
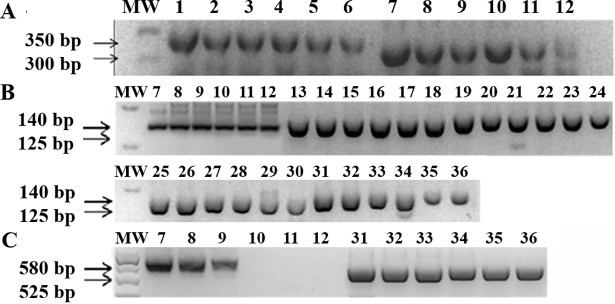
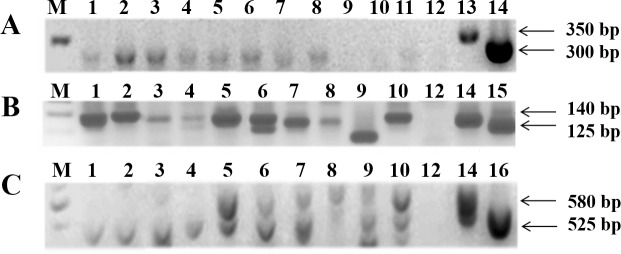
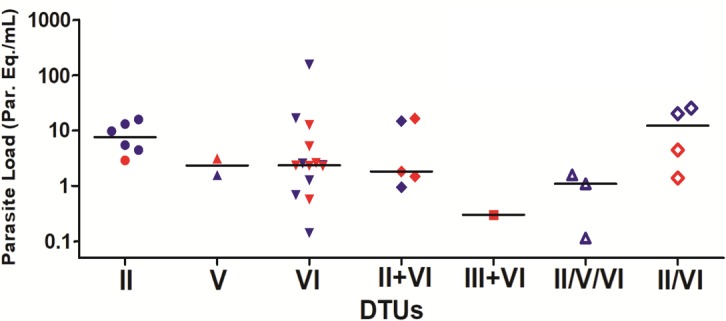
Chagas disease is still a major public health issue in many Latin American countries. One of the current major challenges is to find an association between Trypanosoma cruzi discrete typing units (DTUs) and clinical manifestations of the disease. In this study, we used a multilocus conventional PCR and quantitative real time PCR (qPCR) approaches to perform the molecular typing and parasite load quantification directly from blood specimens of 65 chronic Chagas disease patients. All patients were recruited at the same health center, but their place of birth were widely distributed in different geographic regions of Brazil. Of the 65 patients, 35 (53.8%) presented positive amplification by real time qPCR, being 20 (30.7%) with the clinical indeterminate form and 15 (23.1%) with the cardiac form of the disease. The parasite load median for all positive patients was 2.54 [1.43-11.14] parasite equivalents/mL (par. Eq./mL), with the load ranging from 0.12 to 153.66 par. Eq./mL. Noteworthy, the parasite load was significantly higher in patients over 70 years old (median 20.05 [18.29-86.86] par. Eq./mL). Using guanidine-EDTA blood samples spiked with reference T. cruzi strains, belonging to the six DTUs, it was possible to genotype the parasite up to 0.5 par. Eq./mL, with high specificity. Of the patients with positive qPCR, it was possible to identify the T. cruzi DTU in 28 patients (80%). For the remaining patients (20%), at least a partial result was obtained. Analysis of specimens showed prevalences of TcVI, TcII and mixed infection TcVI+TcII equal to 40%, 17.1% and 14.3%, respectively. In addition, two patients were infected by TcV, and one patient was coinfected by TcIII+TcVI, These last three patients were in stage A of chronic chagasic cardiomyopathy (CCC), and they were born at the Bahia State (northeast region of Brazil). When T. cruzi genotypes were compared with the parasite load, more elevated parasite loads were observed in patients infected by TcII in general (parasite load median of 7.56 par. Eq./mL) in comparison to patients infected by TcVI (median of 2.35 par. Eq./mL). However, while the frequency of CCC was 50% in patients infected by TcVI and TcV, only 16.7% of patients infected by TcII evolved to CCC. Taking together, our results contribute to update the epidemiological knowledge of T. cruzi DTUs in Brazil, and highlight the age of patient and infection by TcII as important features that lead to the observation of higher parasitemia levels.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Coura JR, Viñas PA. Chagas disease: a new worldwide challenge. Nature. 2010; 465: S6—S7. 10.1038/nature09221 - DOI - PubMed
-
- World Health Organization (WHO). Chagas disease (American trypanosomiasis). 2015. <http://www.who.int/mediacentre/factsheets/fs340/en/>. Acessed in 06/16/2015
-
- Coura JR, Dias JC. Epidemiology, control and surveillance of Chagas disease: 100 years after its discovery. Mem Inst Oswaldo Cruz. 2009; 104 Suppl 1:31–40. - PubMed
-
- Rassi Jr A, Rassi A, Marin-Neto JA. Chagas disease. Lancet. 2010; 375: 1388–402. 10.1016/S0140-6736(10)60061-X - DOI - PubMed
-
- Zingales B., Miles M.A., Campbell D.A., Tibayrenc M., Macedo A.M., Teixeira M.M., et al. The revised Trypanosoma cruzi subspecific nomenclature: Rationale, epidemiological relevance and research applications. Infect Genet Evol. 2012; 12(2): 240–53. 10.1016/j.meegid.201112009 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical