Monitoring and detection of leprosy patients in Southwest China: A retrospective study, 2010-2014
- PMID: 30061618
- PMCID: PMC6065315
- DOI: 10.1038/s41598-018-29753-4
Monitoring and detection of leprosy patients in Southwest China: A retrospective study, 2010-2014
Abstract
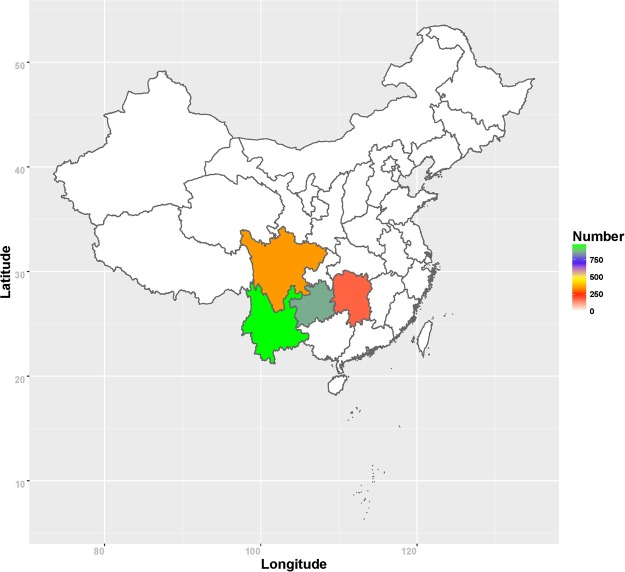
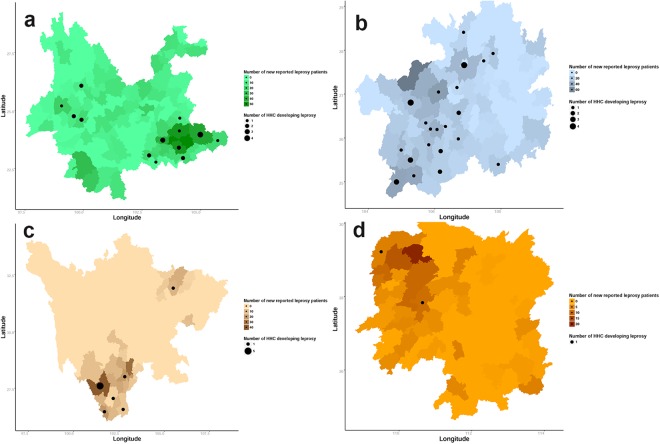
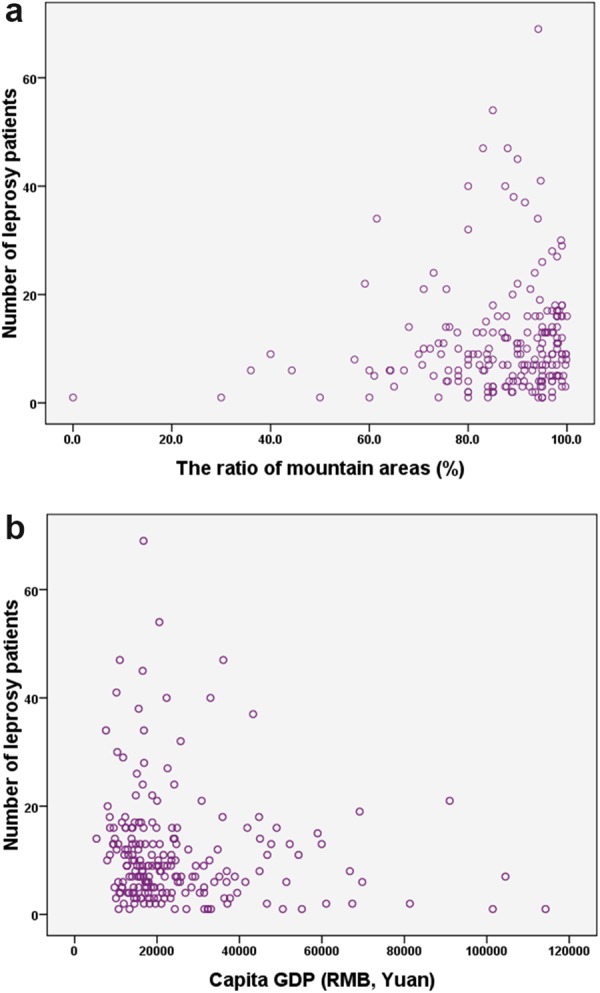
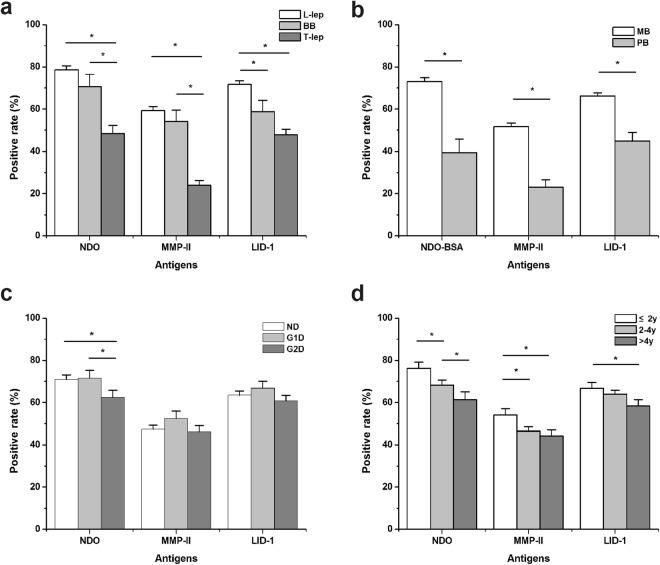
More than 100 counties, mainly in southwest China, report incidence rates of leprosy >1/100,000. The current study analysed the epidemiology of leprosy in southwest China to improve our understanding of the transmission pattern and improve control programs. 207 counties were selected in southwest China. Leprosy patients and their household contacts were recruited. The data from the medical interview and the serological antileprosy antibody of the leprosy patients were analysed. A total of 2,353 new cases of leprosy were interviewed. The distribution of leprosy patients was partly associated with local natural and economic conditions, especially several pocket areas. A total of 53 from 6643 household contacts developed leprosy, and the incidence rate of leprosy in the household contacts was 364/100,000 person-years. We found that NDO-BSA attained higher positive rates than MMP-II and LID-1 regardless of clinical types, disability and infection time in leprosy patients. By means of combination of antigens, 88.4% patients of multibacillary leprosy were detected, in contrast to 59.9% in paucibacillary leprosy. Household contacts should be given close attention for the early diagnosis, disruption of disease transmission and precise control. Applications of serology for multi-antigens were recommended for effective coverage and monitoring in leprosy control.
Conflict of interest statement
The authors declare no competing interests.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical