Adverse events following single dose treatment of lymphatic filariasis: Observations from a review of the literature
- PMID: 29768412
- PMCID: PMC5973625
- DOI: 10.1371/journal.pntd.0006454
Adverse events following single dose treatment of lymphatic filariasis: Observations from a review of the literature
Abstract
Background: WHO's Global Programme to Eliminate Lymphatic Filariasis (LF) uses mass drug administration (MDA) of anthelmintic medications to interrupt LF transmission in endemic areas. Recently, a single dose combination of ivermectin (IVM), diethylcarbamazine (DEC), and albendazole (ALB) was shown to be markedly more effective than the standard two-drug regimens (DEC or IVM, plus ALB) for achieving long-term clearance of microfilaremia.
Objective and methods: To provide context for the results of a large-scale, international safety trial of MDA using triple drug therapy, we searched Ovid Medline for studies published from 1985-2017 that reported adverse events (AEs) following treatment of LF with IVM, DEC, ALB, or any combination of these medications. Studies that reported AE rates by treatment group were included.
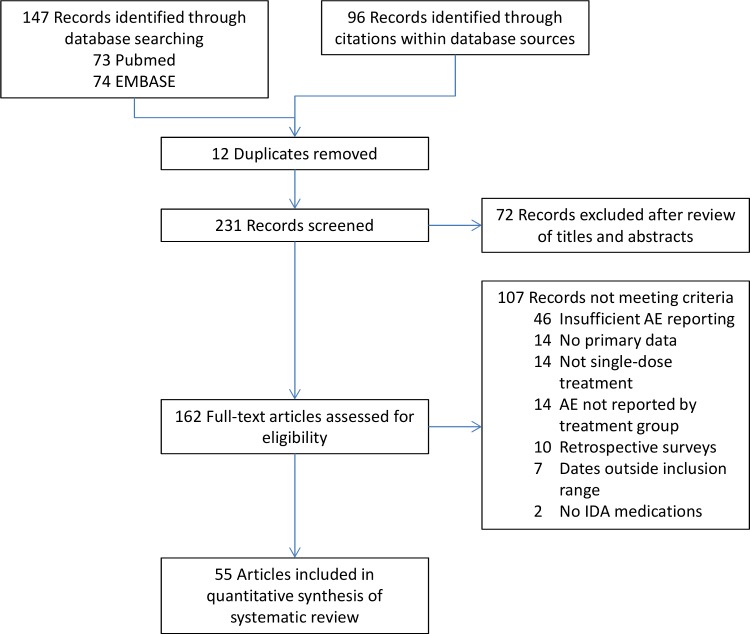
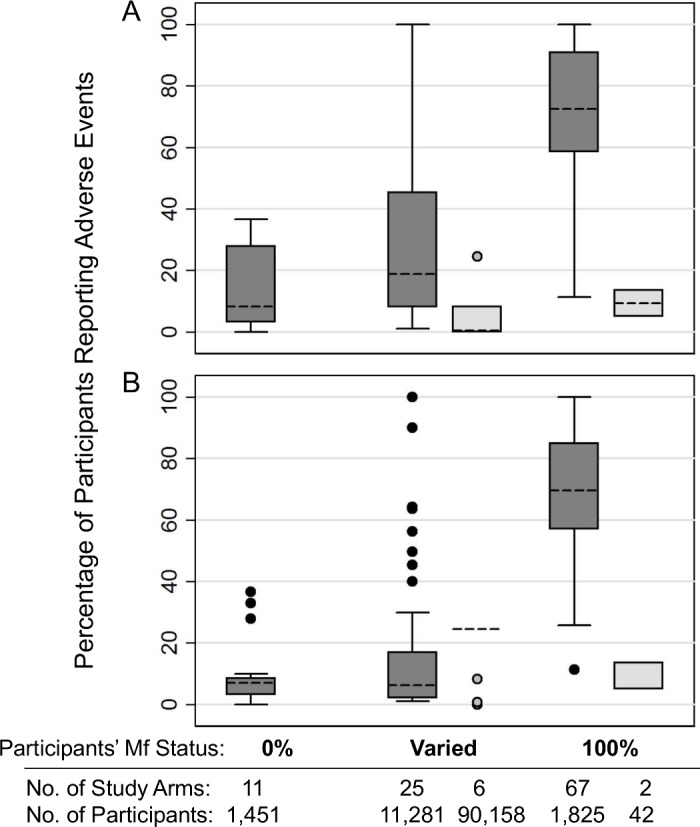
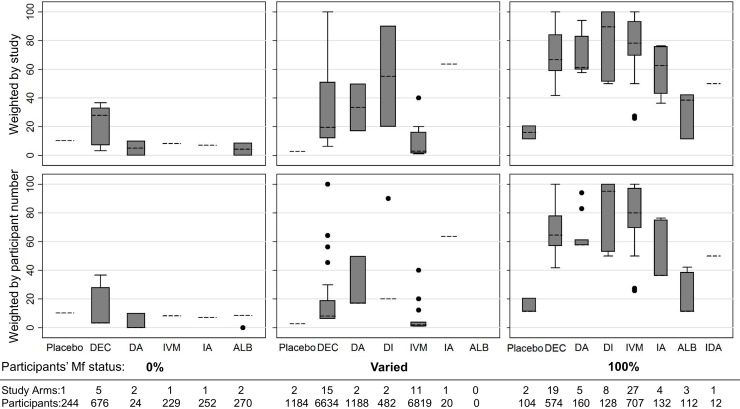
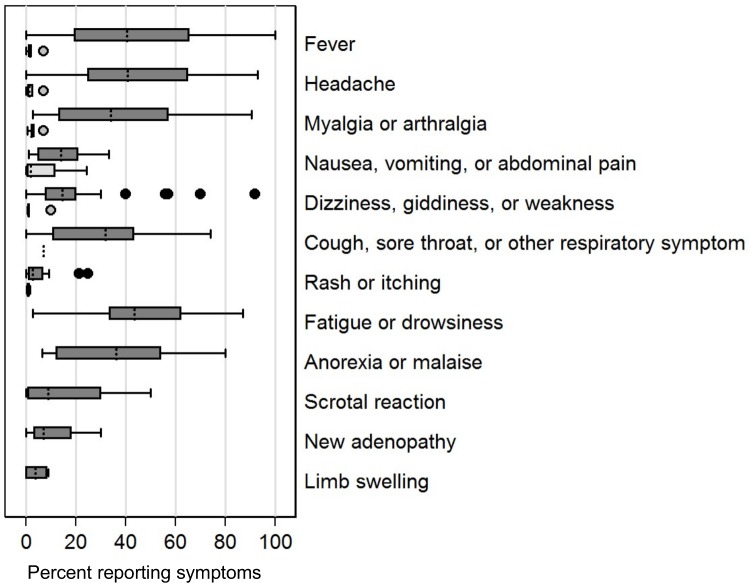
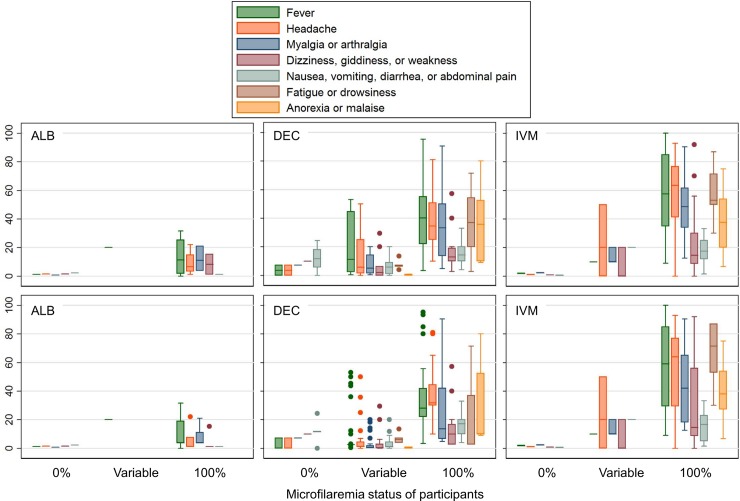
Findings: We reviewed 162 published manuscripts, 55 of which met inclusion criteria. Among these, 34 were clinic or hospital-based clinical trials, and 21 were community-based studies. Reported AE rates varied widely. The median AE rate following DEC or IVM treatment was greater than 60% among microfilaremic participants and less than 10% in persons without microfilaremia. The most common AEs reported were fever, headache, myalgia or arthralgia, fatigue, and malaise.
Interpretation: Mild to moderate systemic AEs related to death of microfilariae are common following LF treatment. Post-treatment AEs are transient and rarely severe or serious. Comparison of AE rates from different community studies is difficult due to inconsistent AE reporting, varied infection rates, and varied intensity of follow-up. A more uniform approach for assessing and reporting AEs in LF community treatment studies would be helpful.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Ichimori K, King JD, Engels D, Yajima A, Mikhailov A, Lammie P, et al. Global programme to eliminate lymphatic filariasis: the processes underlying programme success. PLoS neglected tropical diseases. 2014;8(12):e3328 Epub 2014年12月17日. doi: 10.1371/journal.pntd.0003328 ; PubMed Central PMCID: PMCPmc4263400. - DOI - PMC - PubMed
-
- WHO. Preventive chemotherapy in human helminthiasis: coordinated use of anthelminthic drugs in control interventions: a manual for health professionals and programme managers Geneva, Switzerland: WHO Press; 2006.
-
- Summary of global update on preventive chemotherapy implementation in 2016: crossing the billion. Wkly Epidemiol Rec. 2017;92(40):589–93. . - PubMed
-
- Tisch DJ, Michael E, Kazura JW. Mass chemotherapy options to control lymphatic filariasis: a systematic review. Lancet Infectious Diseases. 2005;5(8):514–23. doi: 10.1016/S1473-3099(05)70192-4. WOS:000231033200020. - DOI - PubMed
-
- Horton J, Witt C, Ottesen EA, Lazdins JK, Addiss DG, Awadzi K, et al. An analysis of the safety of the single dose, two drug regimens used in programmes to eliminate lymphatic filariasis. Parasitology. 2000;121 Suppl:S147–60. Epub 2001年06月02日. . - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous