Longitudinal change in the serology of antibodies to Chlamydia trachomatis pgp3 in children residing in a trachoma area
- PMID: 29476106
- PMCID: PMC5824943
- DOI: 10.1038/s41598-018-21127-0
Longitudinal change in the serology of antibodies to Chlamydia trachomatis pgp3 in children residing in a trachoma area
Abstract
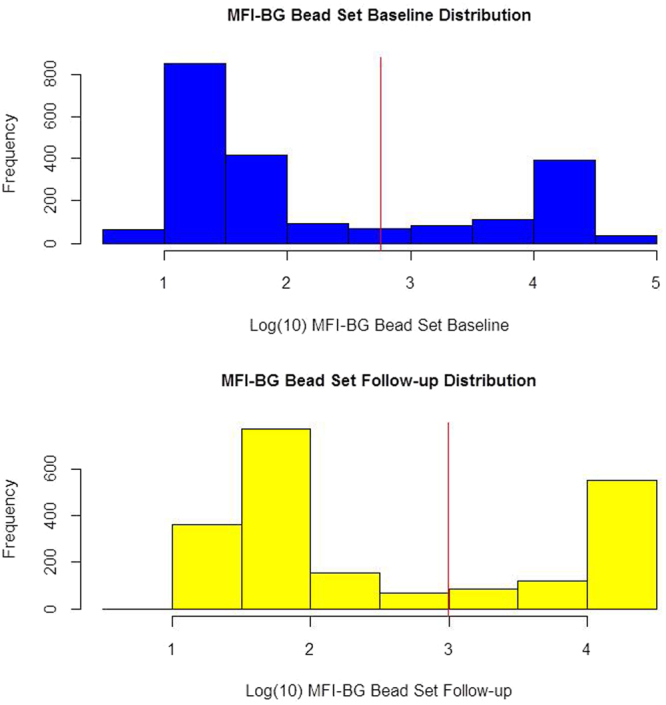
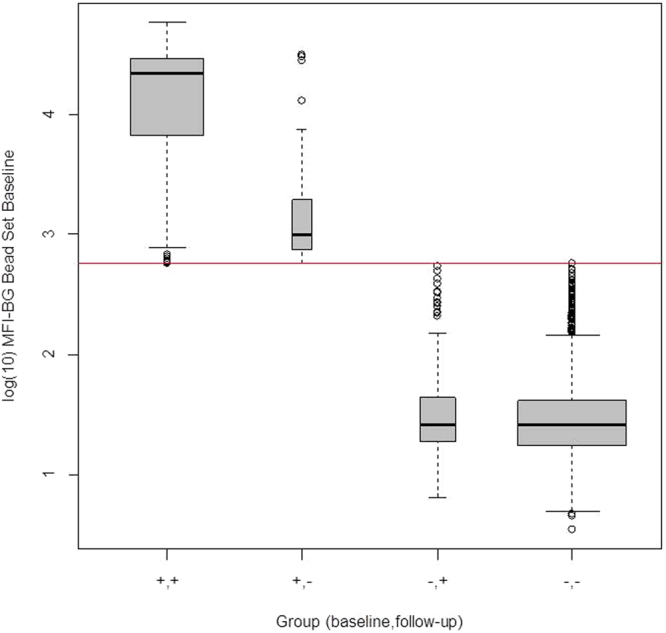
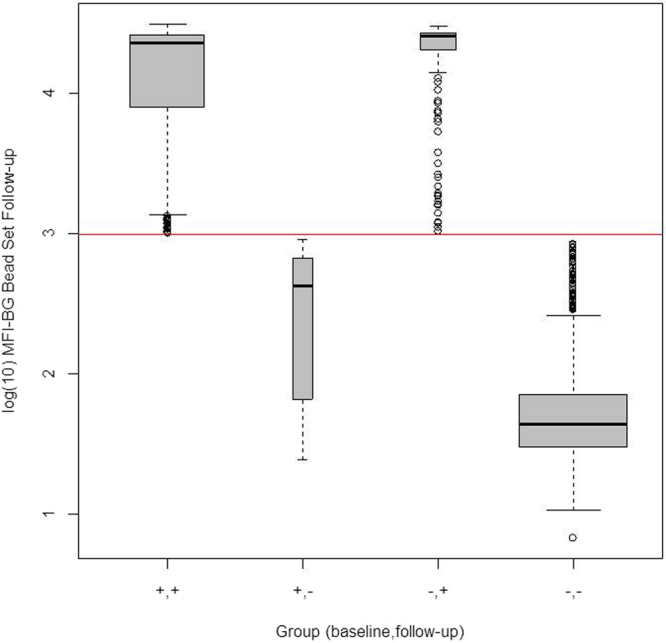
A serologic test for antibodies to chlamydial antigen pgp3 may be a useful tool for trachoma surveillance. However, little is known about the stability of antibody status over time, or factors associated with seroreversion/conversion. A cohort of 2,111 children ages 1-9 years in Tanzania were followed for one year in the absence of mass azithromycin. At baseline and follow-up, they were evaluated for trachoma, chlamydial infection, and antibodies to chlamydial antigen pgp3. At baseline, 31% of children were seropositive for pgp3 antibodies and 6.4% seroreverted to negative over one year. Of those seronegative, 9.8% seroconverted over the year. The seroreverters had lower baseline mean fluorescence intensity (MFI-BG) values compared to the seropositives who remained positive (Odds Ratio = 0.04 for every unit increase in log10MFI-BG, 95% CI = 0.02-0.09), and were more likely to live in communities with trachoma <5% (p < 0.008). While seroconversion was expected, seroreversion was unexpected. The low seroprevalence rate reported from low endemic areas may be due to seroreversion as well as lack of exposure.
Conflict of interest statement
The authors declare no competing interests.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- World_Health_Organization. in WHA51.11 (ed World_Health_Assembly) (1998).
-
- World_Health_Organization. Technical Consultation on Trachoma Surveillance. 1–23 (World Health Organization Press Geneva, Switzerland, 2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources