Population-Based Surveillance of Birth Defects Potentially Related to Zika Virus Infection - 15 States and U.S. Territories, 2016
- PMID: 29370151
- PMCID: PMC5812309
- DOI: 10.15585/mmwr.mm6703a2
Population-Based Surveillance of Birth Defects Potentially Related to Zika Virus Infection - 15 States and U.S. Territories, 2016
Abstract
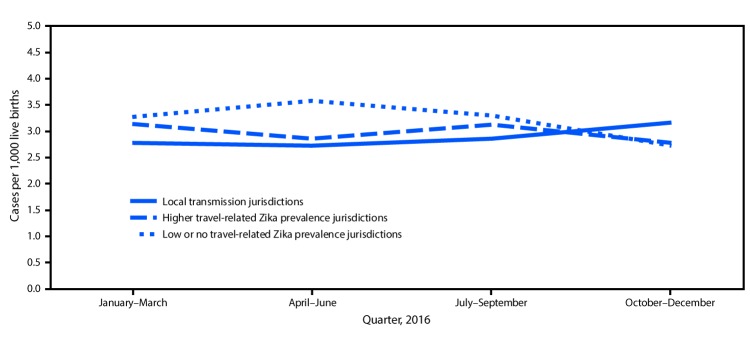
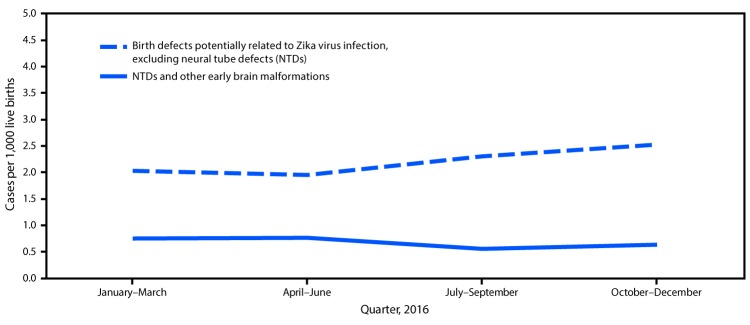
Zika virus infection during pregnancy can cause serious birth defects, including microcephaly and brain abnormalities (1). Population-based birth defects surveillance systems are critical to monitor all infants and fetuses with birth defects potentially related to Zika virus infection, regardless of known exposure or laboratory evidence of Zika virus infection during pregnancy. CDC analyzed data from 15 U.S. jurisdictions conducting population-based surveillance for birth defects potentially related to Zika virus infection.* Jurisdictions were stratified into the following three groups: those with 1) documented local transmission of Zika virus during 2016; 2) one or more cases of confirmed, symptomatic, travel-associated Zika virus disease reported to CDC per 100,000 residents; and 3) less than one case of confirmed, symptomatic, travel-associated Zika virus disease reported to CDC per 100,000 residents. A total of 2,962 infants and fetuses (3.0 per 1,000 live births; 95% confidence interval [CI] = 2.9-3.2) (2) met the case definition.† In areas with local transmission there was a non-statistically significant increase in total birth defects potentially related to Zika virus infection from 2.8 cases per 1,000 live births in the first half of 2016 to 3.0 cases in the second half (p = 0.10). However, when neural tube defects and other early brain malformations (NTDs)§ were excluded, the prevalence of birth defects strongly linked to congenital Zika virus infection increased significantly, from 2.0 cases per 1,000 live births in the first half of 2016 to 2.4 cases in the second half, an increase of 29 more cases than expected (p = 0.009). These findings underscore the importance of surveillance for birth defects potentially related to Zika virus infection and the need for continued monitoring in areas at risk for Zika.
Conflict of interest statement
No conflicts of interest were reported.
Figures
{kind=link}
{kind=link}
References
-
- CDC. Zika virus: 2016 cases counts in the US. Laboratory-confirmed symptomatic Zika virus disease cases and presumptive viremic blood donors reported to ArboNET by states and territories—United States, 2016. Atlanta, GA: US Department of Health and Human Services, CDC; 2017. https://www.cdc.gov/zika/reporting/2016-case-counts.html
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous