Treatment of adult chronic indeterminate Chagas disease with benznidazole and three E1224 dosing regimens: a proof-of-concept, randomised, placebo-controlled trial
- PMID: 29352704
- PMCID: PMC7612561
- DOI: 10.1016/S1473-3099(17)30538-8
Treatment of adult chronic indeterminate Chagas disease with benznidazole and three E1224 dosing regimens: a proof-of-concept, randomised, placebo-controlled trial
Abstract
Background: Chagas disease is a major neglected vector-borne disease. In this study, we investigated the safety and efficacy of three oral E1224 (a water-soluble ravuconazole prodrug) regimens and benznidazole versus placebo in adult chronic indeterminate Chagas disease.
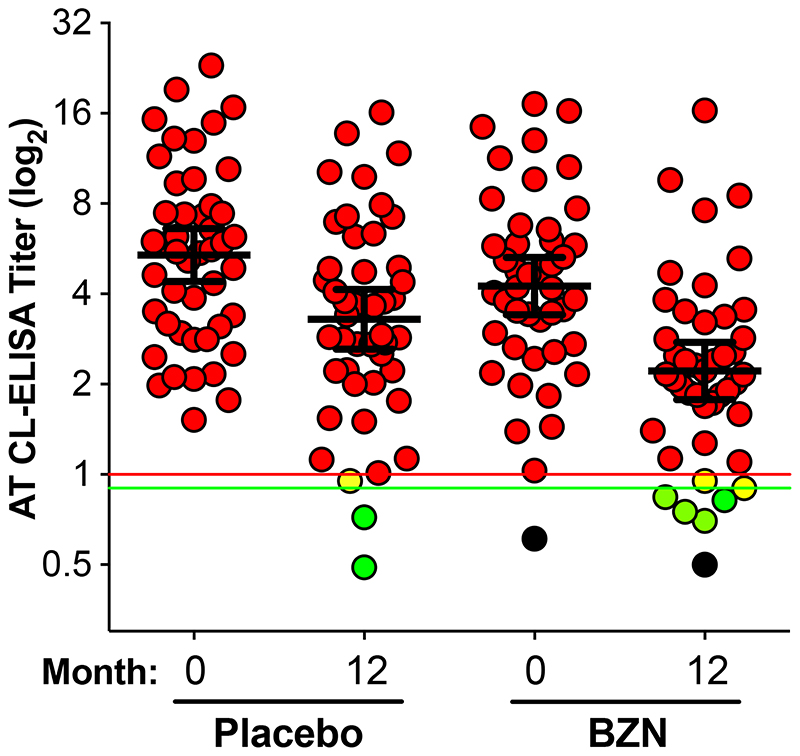
Method: In this proof-of-concept, double-blind, randomised phase 2 clinical trial, we recruited adults (18-50 years) with confirmed diagnosis of Trypanosoma cruzi infection from two outpatient units in Bolivia. Patients were randomised with a computer-generated randomisation list, which was stratified by centre and used a block size of ten. Patients were randomly assigned (1:1:1:1:1) to five oral treatment groups: high-dose E1224 (duration 8 weeks, total dose 4000 mg), low-dose E1224 (8 weeks, 2000 mg), short-dose E1224 (4 weeks + 4 weeks placebo, 2400 mg), benznidazole (60 days, 5 mg/kg per day), or placebo (8 weeks, E1224-matched tablets). Double-blinding was limited to the E1224 and placebo arms, and assessors were masked to all treatment allocations. The primary efficacy endpoint was parasitological response to E1224 at the end of treatment, assessed by PCR. The secondary efficacy endpoints were parasitological response to benznidazole at end of treatment, assessed by PCR; sustainability of parasitological response until 12 months; parasite clearance and changes in parasite load; incidence of conversion to negative response in conventional and non-conventional (antigen trypomastigote chemiluminescent ELISA [AT CL-ELISA]) serological response; changes in levels of biomarkers; and complete response. The primary analysis population consisted of all randomised patients by their assigned treatment arms. This trial is registered with ClinicalTrials.gov, number NCT01489228.
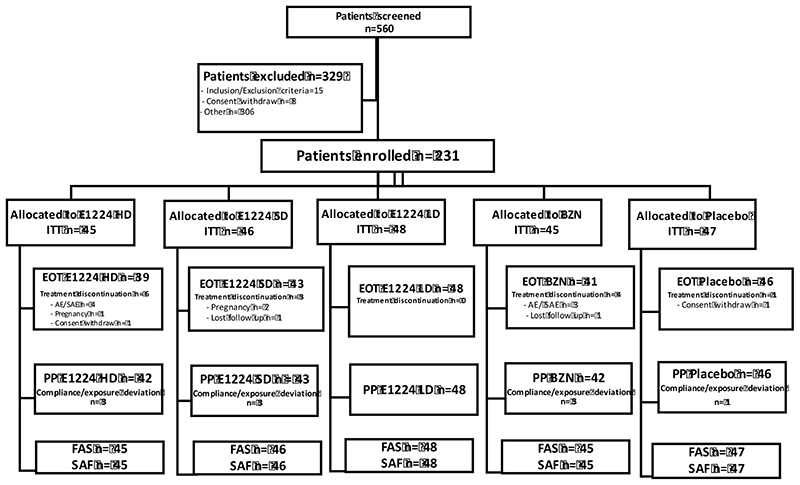
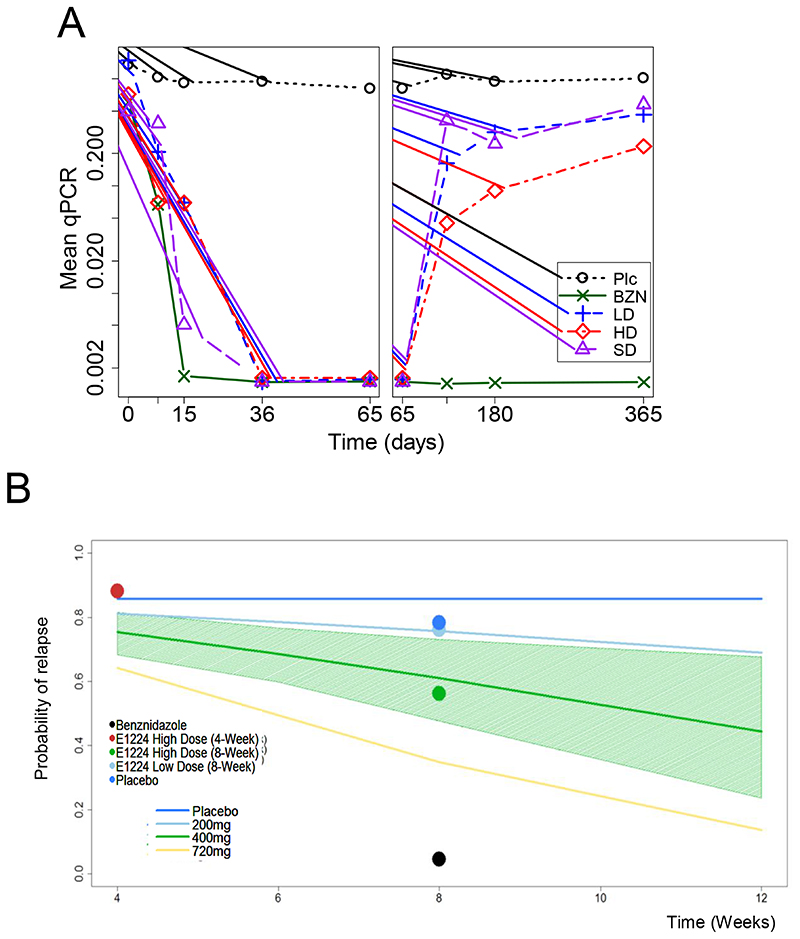
Findings: Between July 19, 2011, and July 26, 2012, we screened 560 participants with confirmed Chagas disease, of whom 231 were enrolled and assigned to high-dose E1224 (n=45), low-dose E1224 (n=48), short-dose E1224 (n=46), benznidazole (n=45), or placebo (n=47). Parasite clearance was observed with E1224 during the treatment phase, but no sustained response was seen with low-dose and short-dose regimens, whereas 13 patients (29%, 95% CI 16·4-44·3) had sustained response with the high-dose regimen compared with four (9%, 2·4-20·4) in the placebo group (p<0·0001). Benznidazole had a rapid and sustained effect on parasite clearance, with 37 patients (82%, 67·9-92·0) with sustained response at 12-month follow-up. After 1 week of treatment, mean quantitative PCR repeated measurements showed a significant reduction in parasite load in all treatment arms versus placebo. Parasite levels in the low-dose and short-dose E1224 groups gradually returned to placebo levels. Both treatments were well tolerated. Reversible, dose-dependent liver enzyme increases were seen with E1224 and benznidazole. 187 (81%) participants developed treatment-emergent adverse events and six (3%) developed treatment-emergent serious adverse events. Treatment-emergent adverse events were headaches, nausea, pruritus, peripheral neuropathy, and hypersensitivity.
Interpretation: E1224 is the first new chemical entity developed for Chagas disease in decades. E1224 displayed a transient, suppressive effect on parasite clearance, whereas benznidazole showed early and sustained efficacy until 12 months of follow-up. Despite PCR limitations, our results support increased diagnosis and access to benznidazole standard regimen, and provide a development roadmap for novel benznidazole regimens in monotherapy and in combinations with E1224.
Funding: Drugs for Neglected Diseases initiative.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
{kind=link}
{kind=link}
{kind=link}
Comment in
-
The long road towards a safe and effective treatment of chronic Chagas disease.Urbina JA. Urbina JA. Lancet Infect Dis. 2018 Apr;18(4):363-365. doi: 10.1016/S1473-3099(17)30535-2. Epub 2018 Jan 16. Lancet Infect Dis. 2018. PMID: 29352705 No abstract available.
-
Chronic Chagas disease: therapeutic protocols and efficacy endpoints.Gonçalves RV, Novaes RD. Gonçalves RV, et al. Lancet Infect Dis. 2018 Jul;18(7):719-720. doi: 10.1016/S1473-3099(18)30342-6. Lancet Infect Dis. 2018. PMID: 29976524 No abstract available.
References
-
- World Health Organization. Chagas disease in Latin America: an epidemiological update based on 2010 estimates. Wkly Epidemiol Rec. 2015;90:33–44. - PubMed
-
- Rassi A, Jr, Rassi A, Marin-Neto JA. Chagas disease. Lancet. 2010;375:1388–402. - PubMed
-
- Diez M, Favaloro L, Bertolotti A, et al. Usefulness of PCR strategies for early diagnosis of Chagas’ disease reactivation and treatment follow-up in heart transplantation. Am J Transplant. 2007;7:1633–40. - PubMed
-
- Castro AM, Luquetti AO, Rassi A, Rassi GG, Chiari E, Galvão LM. Blood culture and polymerase chain reaction for the diagnosis of the chronic phase of human infection with Trypanosoma cruzi. Parasitol Res. 2002;88:894–900. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical