Assessing the feasibility of interrupting the transmission of soil-transmitted helminths through mass drug administration: The DeWorm3 cluster randomized trial protocol
- PMID: 29346377
- PMCID: PMC5773085
- DOI: 10.1371/journal.pntd.0006166
Assessing the feasibility of interrupting the transmission of soil-transmitted helminths through mass drug administration: The DeWorm3 cluster randomized trial protocol
Erratum in
-
Correction: Assessing the feasibility of interrupting the transmission of soil-transmitted helminths through mass drug administration: The DeWorm3 cluster randomized trial protocol.PLOS Neglected Tropical Diseases Staff. PLOS Neglected Tropical Diseases Staff. PLoS Negl Trop Dis. 2018 Jan 31;12(1):e0006253. doi: 10.1371/journal.pntd.0006253. eCollection 2018 Jan. PLoS Negl Trop Dis. 2018. PMID: 29385138 Free PMC article.
Abstract
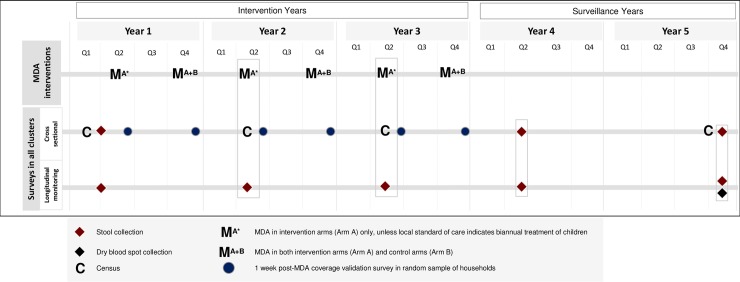
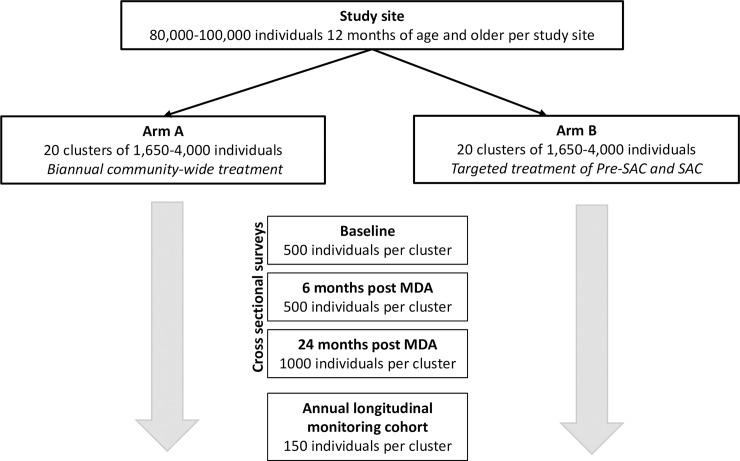
Current control strategies for soil-transmitted helminths (STH) emphasize morbidity control through mass drug administration (MDA) targeting preschool- and school-age children, women of childbearing age and adults in certain high-risk occupations such as agricultural laborers or miners. This strategy is effective at reducing morbidity in those treated but, without massive economic development, it is unlikely it will interrupt transmission. MDA will therefore need to continue indefinitely to maintain benefit. Mathematical models suggest that transmission interruption may be achievable through MDA alone, provided that all age groups are targeted with high coverage. The DeWorm3 Project will test the feasibility of interrupting STH transmission using biannual MDA targeting all age groups. Study sites (population ≥80,000) have been identified in Benin, Malawi and India. Each site will be divided into 40 clusters, to be randomized 1:1 to three years of twice-annual community-wide MDA or standard-of-care MDA, typically annual school-based deworming. Community-wide MDA will be delivered door-to-door, while standard-of-care MDA will be delivered according to national guidelines. The primary outcome is transmission interruption of the STH species present at each site, defined as weighted cluster-level prevalence ≤2% by quantitative polymerase chain reaction (qPCR), 24 months after the final round of MDA. Secondary outcomes include the endline prevalence of STH, overall and by species, and the endline prevalence of STH among children under five as an indicator of incident infections. Secondary analyses will identify cluster-level factors associated with transmission interruption. Prevalence will be assessed using qPCR of stool samples collected from a random sample of cluster residents at baseline, six months after the final round of MDA and 24 months post-MDA. A smaller number of individuals in each cluster will be followed with annual sampling to monitor trends in prevalence and reinfection throughout the trial.
Trial registration: ClinicalTrials.gov NCT03014167.
Conflict of interest statement
The study is funded by the Bill and Melinda Gates Foundation. The funders reviewed but were not involved in final decisions regarding the study design and trial procedures. The funders were not involved in the decision to publish the manuscript and will have no role in data collection, analysis or publication of study results.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Hotez P., Helminth Infections: Soil-transmitted Helminth Infections and Schistosomiasis, in Disease Control Priorities in Developing Countries. 2006, World Bank.
-
- Pullan R.L., et al. , Global numbers of infection and disease burden of soil transmitted helminth infections in 2010. Parasit Vectors, 2014. 7: p. 37 doi: 10.1186/1756-3305-7-37 - DOI - PMC - PubMed
-
- WHO, Accelerating Work to Overcome the Global Impact of Neglected Tropical Diseases: A Roadmap for Implementation. 2012, World Health Organization: Geneva
-
- Organization, W.H., Guideline: preventive chemotherapy to control soil-transmitted helminth infections in at-risk population groups 2017, Geneva. 75. - PubMed
-
- Gabrielli A.F., et al. , Preventive chemotherapy in human helminthiasis: theoretical and operational aspects. Trans R Soc Trop Med Hyg, 2011. 105(12): p. 683–93. doi: 10.1016/j.trstmh.2011年08月01日3 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical