Preclinical antivenom-efficacy testing reveals potentially disturbing deficiencies of snakebite treatment capability in East Africa
- PMID: 29045429
- PMCID: PMC5646754
- DOI: 10.1371/journal.pntd.0005969
Preclinical antivenom-efficacy testing reveals potentially disturbing deficiencies of snakebite treatment capability in East Africa
Erratum in
-
Correction: Preclinical antivenom-efficacy testing reveals potentially disturbing deficiencies of snakebite treatment capability in East Africa.Harrison RA, Oluoch GO, Ainsworth S, Alsolaiss J, Bolton F, Arias AS, Gutiérrez JM, Rowley P, Kalya S, Ozwara H, Casewell NR. Harrison RA, et al. PLoS Negl Trop Dis. 2020 Aug 31;14(8):e0008698. doi: 10.1371/journal.pntd.0008698. eCollection 2020 Aug. PLoS Negl Trop Dis. 2020. PMID: 32866144 Free PMC article.
Abstract
Background: Antivenom is the treatment of choice for snakebite, which annually kills an estimated 32,000 people in sub-Saharan Africa and leaves approximately 100,000 survivors with permanent physical disabilities that exert a considerable socioeconomic burden. Over the past two decades, the high costs of the most polyspecifically-effective antivenoms have sequentially reduced demand, commercial manufacturing incentives and production volumes that have combined to create a continent-wide vacuum of effective snakebite therapy. This was quickly filled with new, less expensive antivenoms, many of which are of untested efficacy. Some of these successfully marketed antivenoms for Africa are inappropriately manufactured with venoms from non-African snakes and are dangerously ineffective. The uncertain efficacy of available antivenoms exacerbates the complexity of designing intervention measures to reduce the burden of snakebite in sub-Saharan Africa. The objective of this study was to preclinically determine the ability of antivenoms available in Kenya to neutralise the lethal effects of venoms from the most medically important snakes in East Africa.
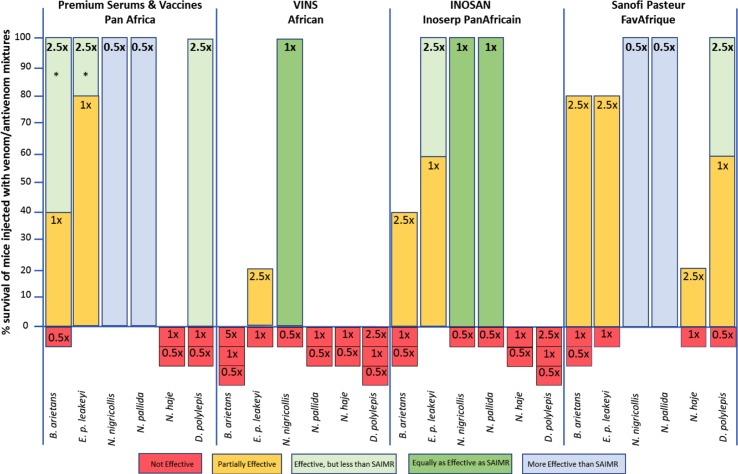
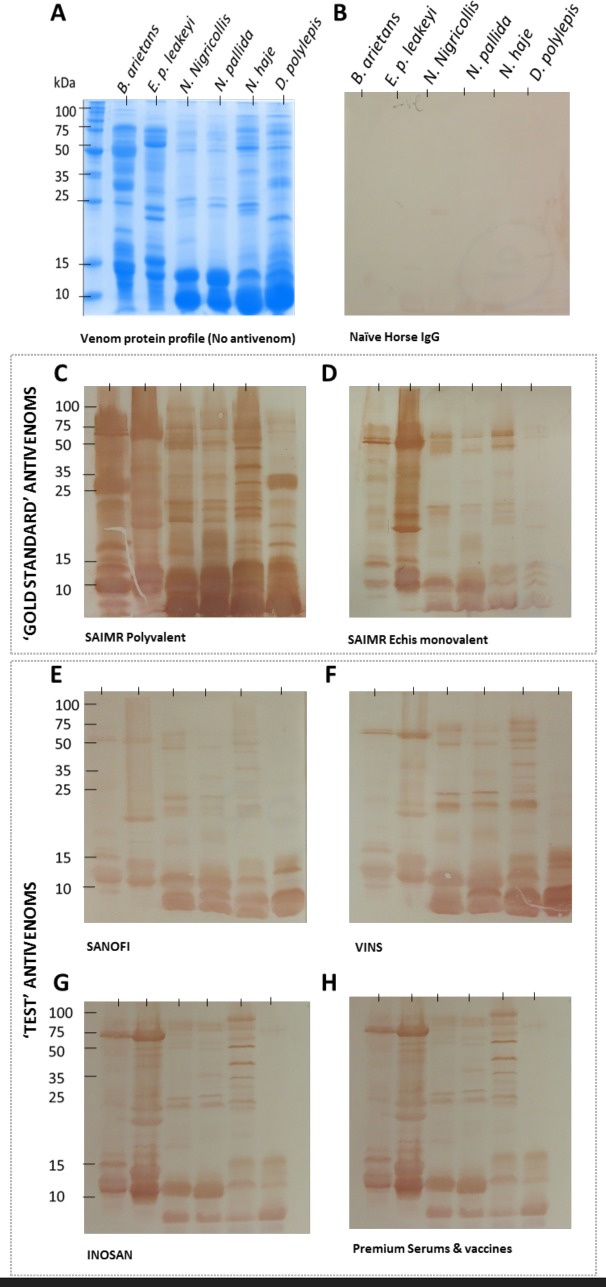
Methods: We collected venom samples from the most medically important snakes in East Africa and determined their toxicity in a mouse model. Using a 'gold standard' comparison protocol, we preclinically tested the comparative venom-neutralising efficacy of four antivenoms available in Kenya with two antivenoms of clinically-proven efficacy. To explain the variant efficacies of these antivenoms we tested the IgG-venom binding characteristics of each antivenom using in vitro IgG titre, avidity and venom-protein specificity assays. We also measured the IgG concentration of each antivenom.
Findings: None of the six antivenoms are preclinically effective, at the doses tested, against all of the most medically important snakes of the region. The very limited snake polyspecific efficacy of two locally available antivenoms is of concern. In vitro assays of the abilities of 'test' antivenom IgGs to bind venom proteins were not substantially different from that of the 'gold standard' antivenoms. The least effective antivenoms had the lowest IgG content/vial.
Conclusions: Manufacture-stated preclinical efficacy statements guide decision making by physicians and antivenom purchasers in sub-Saharan Africa. This is because of the lack of both clinical data on the efficacy of most of the many antivenoms used to treat patients and independent preclinical assessment. Our preclinical efficacy assessment of antivenoms available in Kenya identifies important limitations for two of the most commonly-used antivenoms, and that no antivenom is preclinically effective against all the regionally important snakes. The potential implication to snakebite treatment is of serious concern in Kenya and elsewhere in sub-Saharan Africa, and underscores the dilemma physicians face, the need for clinical data on antivenom efficacy and the medical and societal value of establishing independent preclinical antivenom-efficacy testing facilities throughout the continent.
Conflict of interest statement
None of the authors have competing interests.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Kasturiratne A, Wickremasinghe AR, de Silva N, Gunawardena NK, Pathmeswaran A, Premaratna R, Savioli L, Lalloo DG, de Silva HJ. The global burden of snakebite: a literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS medicine. 2008. November 4;5(11): e218.https://doi.org/10.1371/journal.pmed.0050218. doi: 10.1371/journal.pmed.0050218 - DOI - DOI - PMC - PubMed
-
- Harrison RA, Hargreaves A, Wagstaff SC, Faragher B, Lalloo DG. Snake envenoming: a disease of poverty. PLoS Neglected Tropical Diseases. 2009. December 22;3(12): e569 https://doi.org/10.1371/journal.pntd.0000569. doi: 10.1371/journal.pntd.0000569 - DOI - DOI - PMC - PubMed
-
- Mohapatra B, Warrell DA, Suraweera W, Bhatia P, Dhingra N, Jotkar RM, Rodriguez PS, Mishra K, Whitaker R, Jha P, Million Death Study Collaborators. Snakebite mortality in India: a nationally representative mortality survey. PLoS Neglected Tropical Diseases. 2011. April 12;5(4): e1018.https://doi.org/10.1371/journal.pntd.0001018. doi: 10.1371/journal.pntd.0001018 - DOI - DOI - PMC - PubMed
-
- Harrison RA, Gutiérrez JM. Priority Actions and progress to substantially and sustainably reduce the mortality, morbidity and socioeconomic burden of tropical snakebite. Toxins. 2016. November 24;8(12): 351.https://doi.org/10.3390/toxins8120351. - DOI - PMC - PubMed
-
- Kofi Annan Foundation. Snakebites in Africa: Challenges and Solutions. 2017 https://www.google.co.uk/search?q=Kofi+Annan+Foundation.+Snakebites+in+A...
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous