Visceral leishmaniasis relapse hazard is linked to reduced miltefosine exposure in patients from Eastern Africa: a population pharmacokinetic/pharmacodynamic study
- PMID: 28961737
- PMCID: PMC5890687
- DOI: 10.1093/jac/dkx283
Visceral leishmaniasis relapse hazard is linked to reduced miltefosine exposure in patients from Eastern Africa: a population pharmacokinetic/pharmacodynamic study
Abstract
Background: Low efficacy of miltefosine in the treatment of visceral leishmaniasis was recently observed in Eastern Africa.
Objectives: To describe the pharmacokinetics and establish a pharmacokinetic/pharmacodynamic relationship for miltefosine in Eastern African patients with visceral leishmaniasis, using a time-to-event approach to model relapse of disease.
Methods: Miltefosine plasma concentrations from 95 patients (48 monotherapy versus 47 combination therapy) were included in the population pharmacokinetic model using non-linear mixed effects modelling. Subsequently a time-to-event model was developed to model the time of clinical relapse. Various summary pharmacokinetic parameters (various AUCs, Time > EC50, Time > EC90), normalized within each treatment arm to allow simultaneous analysis, were evaluated as relapse hazard-changing covariates.
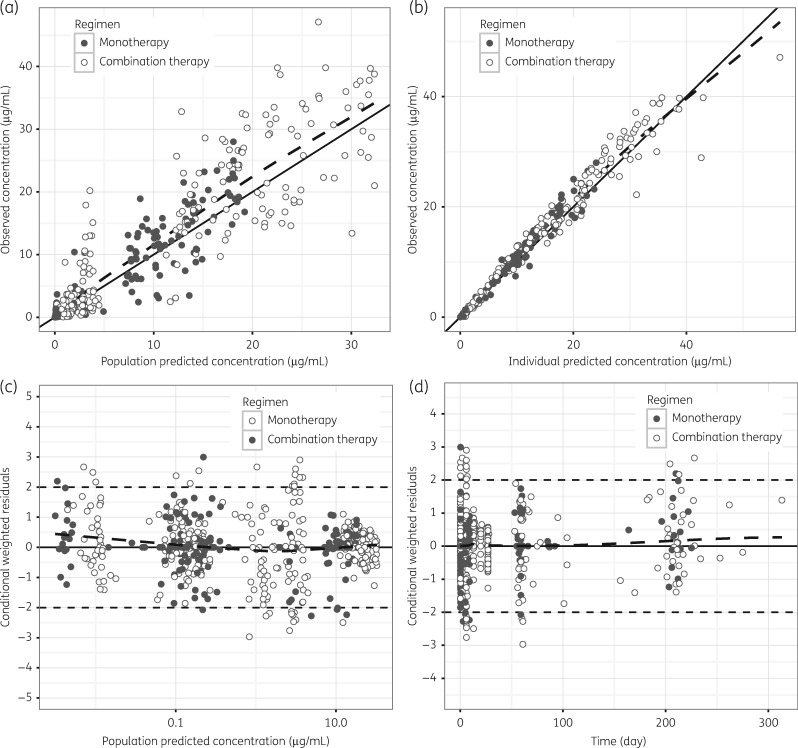
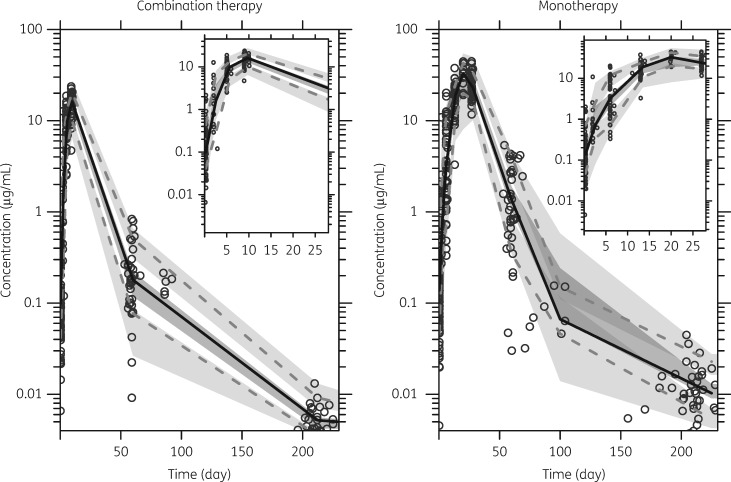
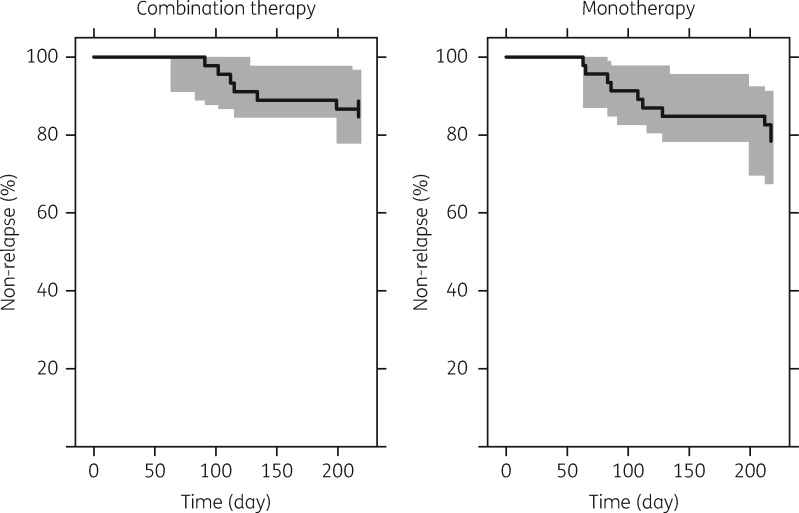
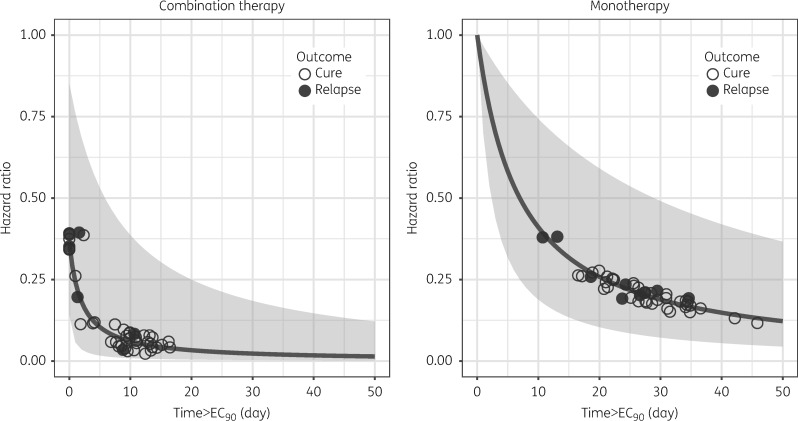
Results: A two-compartment population model with first-order absorption fitted the miltefosine pharmacokinetic data adequately. Relative bioavailability was reduced (-74%, relative standard error 4.7%) during the first week of treatment of the monotherapy arm but only the first day of the shorter combination regimen. Time to the relapse of infection could be described using a constant baseline hazard (baseline 1.8 relapses/year, relative standard error 72.7%). Miltefosine Time > EC90 improved the model significantly when added in a maximum effect function on the baseline hazard (half maximal effect with Time > EC90 6.97 days for monotherapy).
Conclusions: Miltefosine drug exposure was found to be decreased in Eastern African patients with visceral leishmaniasis, due to a (transient) initial lower bioavailability. Relapse hazard was inversely linked to miltefosine exposure. Significantly lower miltefosine exposure was observed in children compared with adults, further urging the need for implementation of dose adaptations for children.
© The Author 2017. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Boelaert M, Meheus F, Sanchez A. et al. The poorest of the poor: a poverty appraisal of households affected by visceral leishmaniasis in Bihar, India. Trop Med Int Health 2009; 14: 639–44. - PubMed
-
- Rijal S, Ostyn B, Uranw S. et al. Increasing failure of miltefosine in the treatment of Kala-azar in Nepal and the potential role of parasite drug resistance, reinfection, or noncompliance. Clin Infect Dis 2013; 56: 1530–8. - PubMed
-
- Dorlo TP, Balasegaram M, Beijnen JH. et al. Miltefosine: a review of its pharmacology and therapeutic efficacy in the treatment of leishmaniasis. J Antimicrob Chemother 2012; 67: 2576–97. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources