Babesiosis Surveillance - Wisconsin, 2001-2015
- PMID: 28683059
- PMCID: PMC5726235
- DOI: 10.15585/mmwr.mm6626a2
Babesiosis Surveillance - Wisconsin, 2001-2015
Abstract
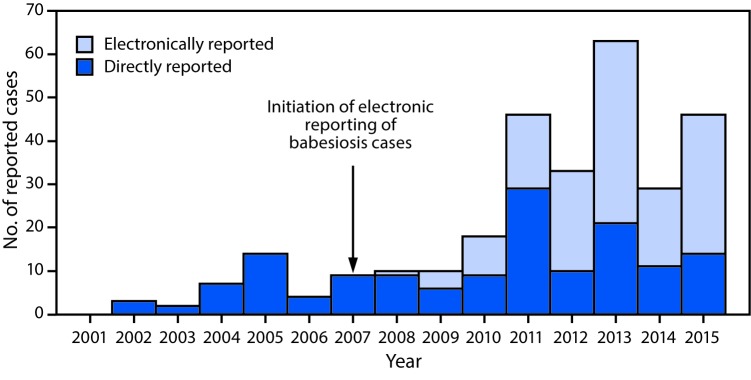
Babesiosis is an emerging zoonotic disease caused primarily by Babesia microti, an intraerythocytic protozoan. Babesia microti, like the causal agents for Lyme disease and anaplasmosis, is endemic to the northeastern and upper midwestern United States where it is usually transmitted by the blacklegged tick, Ixodes scapularis. Although babesiosis is usually a mild to moderate illness, older or immunocompromised persons can develop a serious malaria-like illness that can be fatal without prompt treatment. The most common initial clinical signs and symptoms of babesiosis (fever, fatigue, chills, and diaphoresis) are nonspecific and present diagnostic challenges that can contribute to delays in diagnosis and effective treatment with atovaquone and azithromycin (1). Results of one study revealed a mean delay of 12-14 days from symptom onset to treatment (2). Knowledge of the incidence and geographic distribution of babesiosis can raise the index of clinical suspicion and facilitate more prompt diagnosis and lifesaving treatment (1). The first known case of babesiosis in Wisconsin was detected in 1985 (3), and babesiosis became officially reportable in the state in 2001. Wisconsin babesiosis surveillance data for 2001-2015 were analyzed in 3-year intervals to compare demographic, epidemiologic, and laboratory features among patients with cases of reported babesiosis. To determine possible reasons for an increase in reported Babesia infection, trends in electronic laboratory reporting and diagnosis by polymerase chain reaction testing (PCR) were examined. Between the first and last 3-year analysis intervals, there was a 26-fold increase in the incidence of confirmed babesiosis, in addition to geographic expansion. These trends might be generalizable to other states with endemic disease, similar suburbanization and forest fragmentation patterns, and warming average temperatures (4). Accurate surveillance in states where babesiosis is endemic is necessary to estimate the increasing burden of babesiosis and other tickborne diseases and to develop appropriate public health interventions for prevention and practice.
Conflict of interest statement
Figures
{kind=link}
{kind=link}
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources