qPCR-High resolution melt analysis for drug susceptibility testing of Mycobacterium leprae directly from clinical specimens of leprosy patients
- PMID: 28570560
- PMCID: PMC5453413
- DOI: 10.1371/journal.pntd.0005506
qPCR-High resolution melt analysis for drug susceptibility testing of Mycobacterium leprae directly from clinical specimens of leprosy patients
Abstract
Background: Real-Time PCR-High Resolution Melting (qPCR-HRM) analysis has been recently described for rapid drug susceptibility testing (DST) of Mycobacterium leprae. The purpose of the current study was to further evaluate the validity, reliability, and accuracy of this assay for M. leprae DST in clinical specimens.
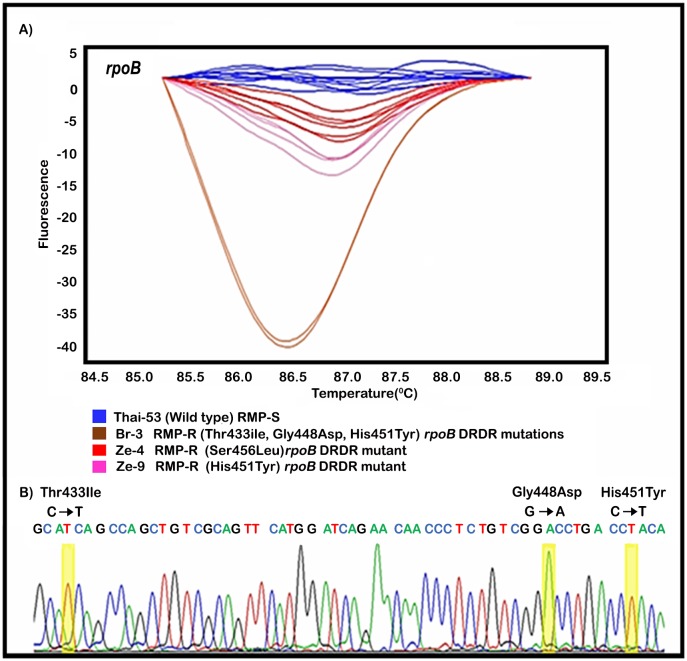
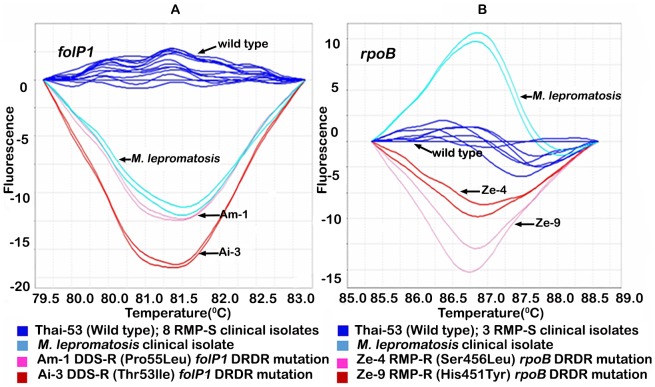
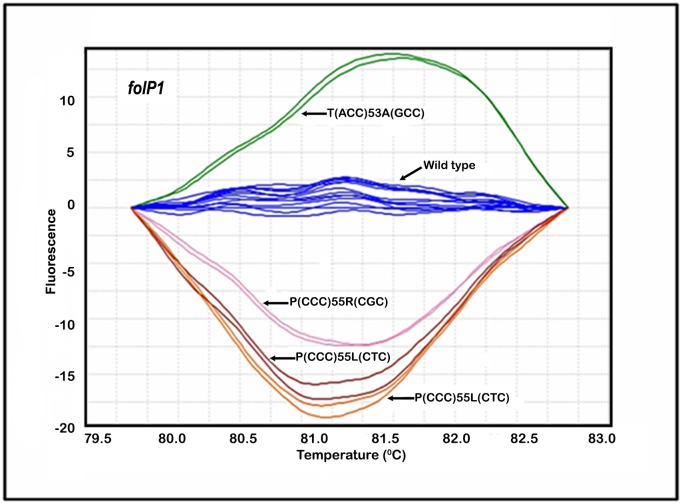
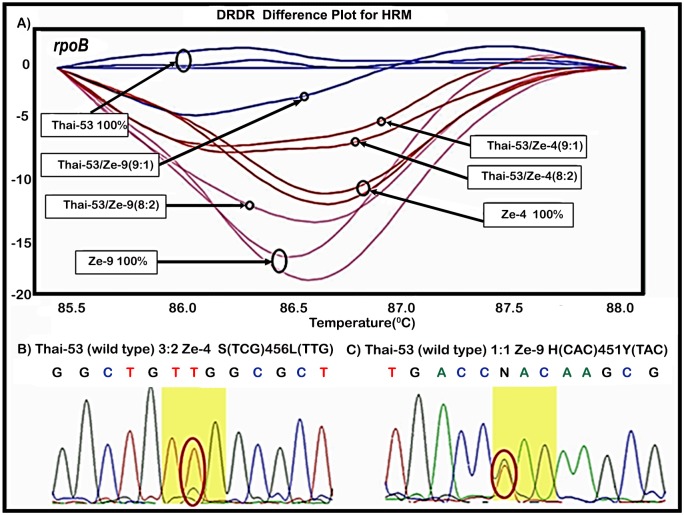
Methodology/principal findings: The specificity and sensitivity for determining the presence and susceptibility of M. leprae to dapsone based on the folP1 drug resistance determining region (DRDR), rifampin (rpoB DRDR) and ofloxacin (gyrA DRDR) was evaluated using 211 clinical specimens from leprosy patients, including 156 multibacillary (MB) and 55 paucibacillary (PB) cases. When comparing the results of qPCR-HRM DST and PCR/direct DNA sequencing, 100% concordance was obtained. The effects of in-house phenol/chloroform extraction versus column-based DNA purification protocols, and that of storage and fixation protocols of specimens for qPCR-HRM DST, were also evaluated. qPCR-HRM results for all DRDR gene assays (folP1, rpoB, and gyrA) were obtained from both MB (154/156; 98.7%) and PB (35/55; 63.3%) patients. All PCR negative specimens were from patients with low numbers of bacilli enumerated by an M. leprae-specific qPCR. We observed that frozen and formalin-fixed paraffin embedded (FFPE) tissues or archival Fite's stained slides were suitable for HRM analysis. Among 20 mycobacterial and other skin bacterial species tested, only M. lepromatosis, highly related to M. leprae, generated amplicons in the qPCR-HRM DST assay for folP1 and rpoB DRDR targets. Both DNA purification protocols tested were efficient in recovering DNA suitable for HRM analysis. However, 3% of clinical specimens purified using the phenol/chloroform DNA purification protocol gave false drug resistant data. DNA obtained from freshly frozen (n = 172), formalin-fixed paraffin embedded (FFPE) tissues (n = 36) or archival Fite's stained slides (n = 3) were suitable for qPCR-HRM DST analysis. The HRM-based assay was also able to identify mixed infections of susceptible and resistant M. leprae. However, to avoid false positives we recommend that clinical specimens be tested for the presence of the M. leprae using the qPCR-RLEP assay prior to being tested in the qPCR-HRM DST and that all specimens demonstrating drug resistant profiles in this assay be subjected to DNA sequencing.
Conclusion/significance: Taken together these results further demonstrate the utility of qPCR-HRM DST as an inexpensive screening tool for large-scale drug resistance surveillance in leprosy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- WHO. World Health Organization Expert Committee on Leprosy. WHO Tech Rep Ser. Geneva: World Health Organization; 2012. p. 1–61. - PubMed
-
- WHO. Chemotherapy of Leprosy for Control Programmes. Report of a World Health Organization Study Group. Geneva: World Health Organization; 1982. p. 1–33. - PubMed
-
- Ellard GA. Rationale of the multidrug regimens recommended by a World Health Organization Study Group on Chemotherapy of Leprosy for Control Programs. Int J Lepr Other Mycobact Dis. 1984;52(3):395–401. - PubMed
-
- WHO. Leprosy: the disease. 2016 [cited 29 of August 2016]. http://www.who.int/lep/leprosy/en/.
-
- Pearson JM, Rees RJ, Waters MF. Sulphone resistance in leprosy. A review of one hundred proven clinical cases. Lancet. 1975;2(7924):69–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous