Human cystic echinococcosis in Morocco: Ultrasound screening in the Mid Atlas through an Italian-Moroccan partnership
- PMID: 28248960
- PMCID: PMC5348040
- DOI: 10.1371/journal.pntd.0005384
Human cystic echinococcosis in Morocco: Ultrasound screening in the Mid Atlas through an Italian-Moroccan partnership
Abstract
Background: Cystic echinococcosis (CE) is a neglected parasitic zoonosis with considerable socioeconomic impact on affected pastoral communities. CE is endemic throughout the Mediterranean, including Morocco, where the Mid Atlas is the most prevalent area for both human and animal infection. The highest hospital annual incidence of human CE is recorded in the provinces of Ifrane and El Hajeb. However, hospital-based statistics likely underestimate the real prevalence of infection, as a proportion of cases never reach medical attention or official records.
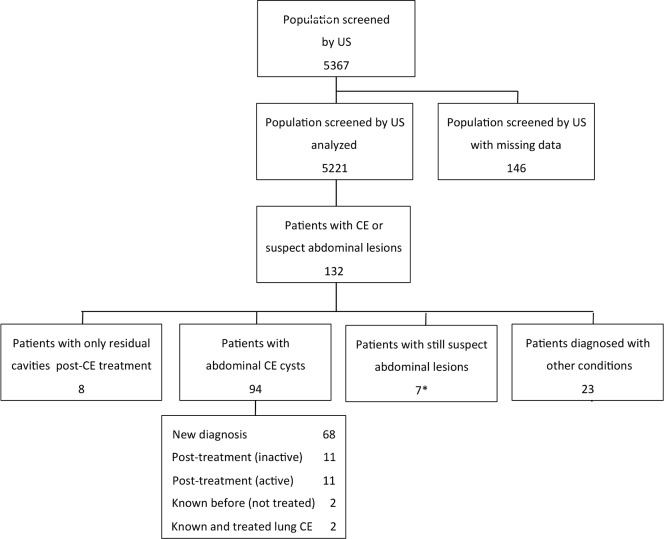
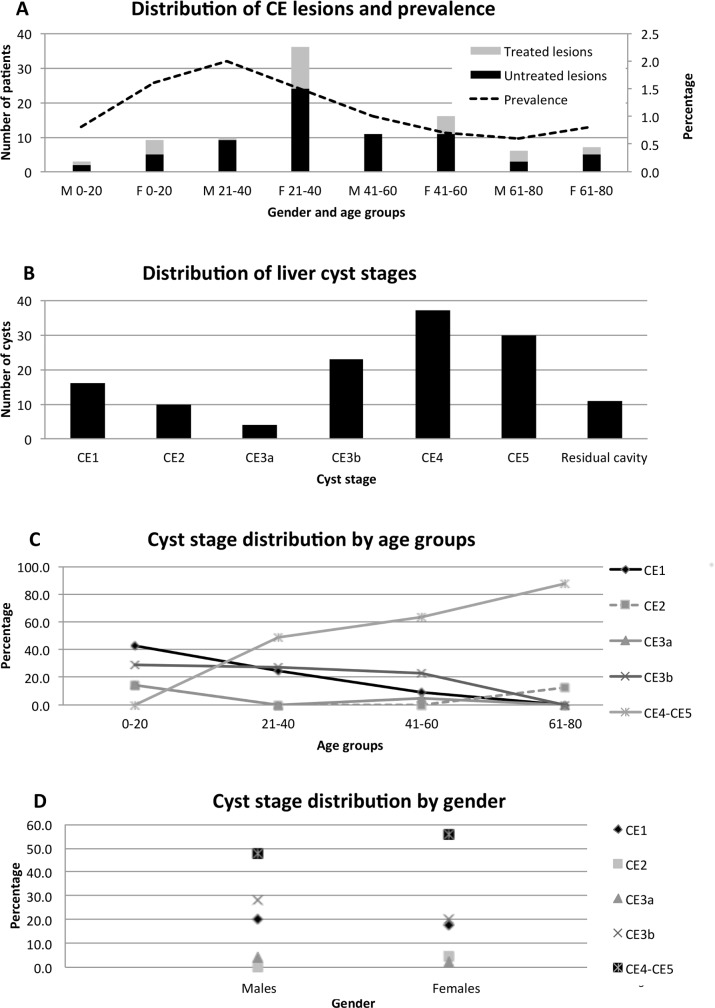
Methodology/principal findings: In 2012, a project on clinical management of CE in Morocco was launched with the aims of estimating the prevalence of human abdominal CE in selected rural communes of the above mentioned provinces using ultrasound (US) screening and training local physicians to implement US-based focused assessment and rational clinical management of CE according to the WHO-IWGE Expert Consensus. A total of 5367 people received abdominal US during four campaigns in April-May 2014. During the campaigns, 24 local general practitioners received >24 hours of hands-on training and 143 health education sessions were organized for local communities. We found an overall CE prevalence of 1.9%, with significantly higher values in the rural communes of Ifrane than El Hajeb (2.6% vs 1.3%; p<0.001). CE cysts were predominantly in inactive stage, especially in older age groups. However, active cysts were present also in adults, indicating acquisition of infection at all ages. Province of residence was the only risk factor consistently associated with CE infection.
Conclusions/significance: Our results show a high prevalence and on-going, likely environmental transmission of CE in the investigated provinces of Morocco, supporting the implementation of control activities in the area by national health authorities and encouraging the acceptance and divulgation of diagnosis and treatment algorithms based on imaging for CE at both national and local level.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Craig P, Budke C, Schantz P, Li T, Qiu J, Yang Y, et al. Human Echinococcosis: A Neglected Disease? Tropical Medicine andHealth. 2007;35(4):283–92.
-
- Derfoufi O, Akawa E, Elmaataoui A, Miss E, Esselmani H, Lyagoubi M, et al. Epidemiological profile of cystic echinococcosis in Morocco from 1980 to 2008. Ann Biol Clin. 2012;70(4):457–61. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous