The Long-Term Safety, Public Health Impact, and Cost-Effectiveness of Routine Vaccination with a Recombinant, Live-Attenuated Dengue Vaccine (Dengvaxia): A Model Comparison Study
- PMID: 27898668
- PMCID: PMC5127514
- DOI: 10.1371/journal.pmed.1002181
The Long-Term Safety, Public Health Impact, and Cost-Effectiveness of Routine Vaccination with a Recombinant, Live-Attenuated Dengue Vaccine (Dengvaxia): A Model Comparison Study
Abstract
Background: Large Phase III trials across Asia and Latin America have recently demonstrated the efficacy of a recombinant, live-attenuated dengue vaccine (Dengvaxia) over the first 25 mo following vaccination. Subsequent data collected in the longer-term follow-up phase, however, have raised concerns about a potential increase in hospitalization risk of subsequent dengue infections, in particular among young, dengue-naïve vaccinees. We here report predictions from eight independent modelling groups on the long-term safety, public health impact, and cost-effectiveness of routine vaccination with Dengvaxia in a range of transmission settings, as characterised by seroprevalence levels among 9-y-olds (SP9). These predictions were conducted for the World Health Organization to inform their recommendations on optimal use of this vaccine.
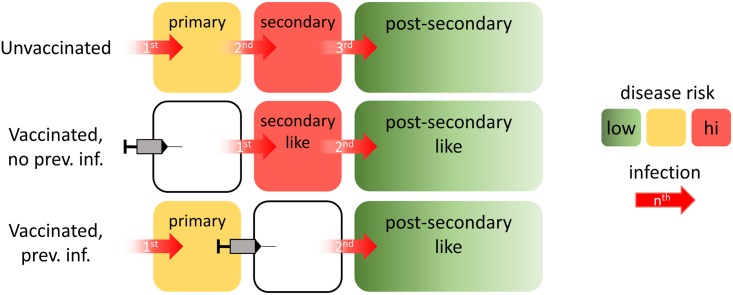
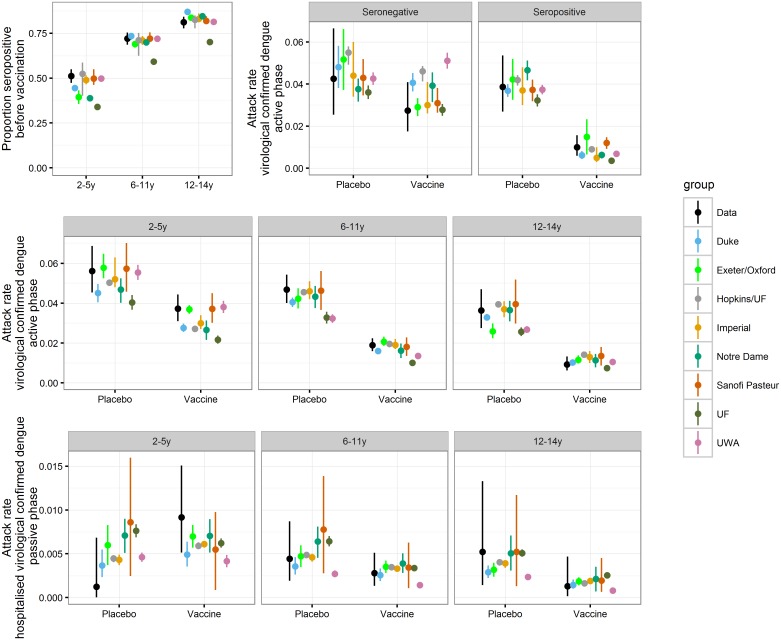
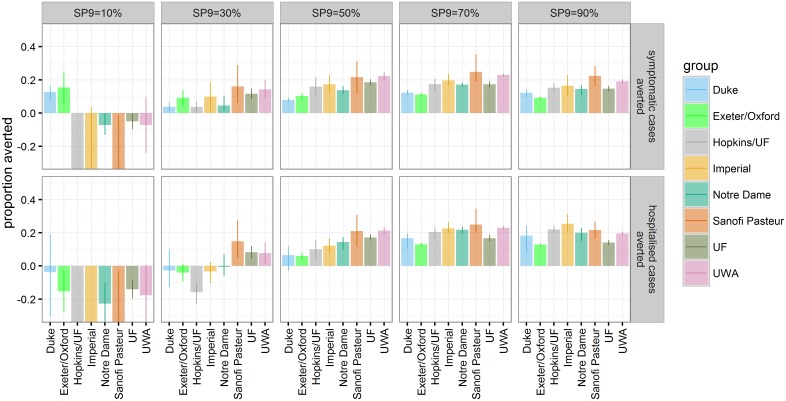
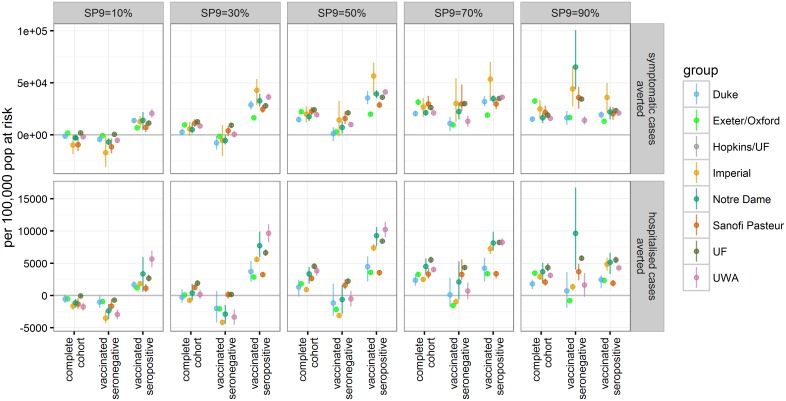
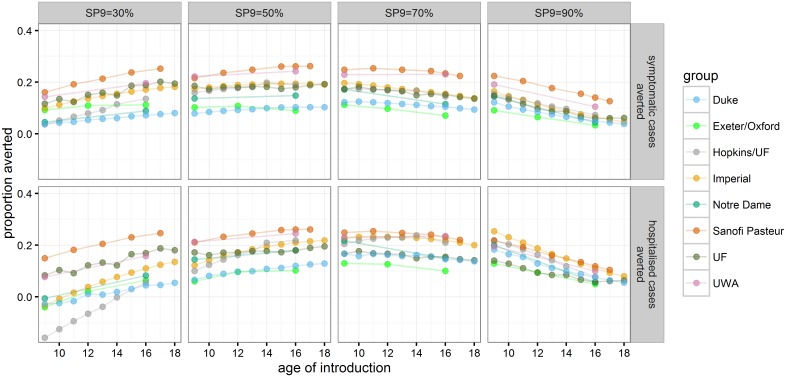
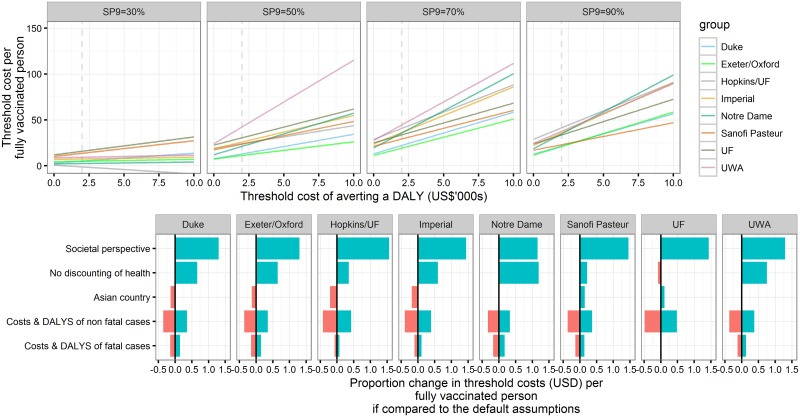
Methods and findings: The models adopted, with small variations, a parsimonious vaccine mode of action that was able to reproduce quantitative features of the observed trial data. The adopted mode of action assumed that vaccination, similarly to natural infection, induces transient, heterologous protection and, further, establishes a long-lasting immunogenic memory, which determines disease severity of subsequent infections. The default vaccination policy considered was routine vaccination of 9-y-old children in a three-dose schedule at 80% coverage. The outcomes examined were the impact of vaccination on infections, symptomatic dengue, hospitalised dengue, deaths, and cost-effectiveness over a 30-y postvaccination period. Case definitions were chosen in accordance with the Phase III trials. All models predicted that in settings with moderate to high dengue endemicity (SP9 ≥ 50%), the default vaccination policy would reduce the burden of dengue disease for the population by 6%-25% (all simulations: -3%-34%) and in high-transmission settings (SP9 ≥ 70%) by 13%-25% (all simulations: 10%- 34%). These endemicity levels are representative of the participating sites in both Phase III trials. In contrast, in settings with low transmission intensity (SP9 ≤ 30%), the models predicted that vaccination could lead to a substantial increase in hospitalisation because of dengue. Modelling reduced vaccine coverage or the addition of catch-up campaigns showed that the impact of vaccination scaled approximately linearly with the number of people vaccinated. In assessing the optimal age of vaccination, we found that targeting older children could increase the net benefit of vaccination in settings with moderate transmission intensity (SP9 = 50%). Overall, vaccination was predicted to be potentially cost-effective in most endemic settings if priced competitively. The results are based on the assumption that the vaccine acts similarly to natural infection. This assumption is consistent with the available trial results but cannot be directly validated in the absence of additional data. Furthermore, uncertainties remain regarding the level of protection provided against disease versus infection and the rate at which vaccine-induced protection declines.
Conclusions: Dengvaxia has the potential to reduce the burden of dengue disease in areas of moderate to high dengue endemicity. However, the potential risks of vaccination in areas with limited exposure to dengue as well as the local costs and benefits of routine vaccination are important considerations for the inclusion of Dengvaxia into existing immunisation programmes. These results were important inputs into WHO global policy for use of this licensed dengue vaccine.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: LC is employed by Sanofi Pasteur. KV is a staff member of the World Health Organization. TAP and GE receive support from GlaxoSmithKline for unrelated work on dengue vaccine modelling. IL, TJH, and CABP have received travel support from Sanofi Pasteur to present other work on dengue vaccine modelling. Sanofi Pasteur has not funded any of their research and was not involved in any research decisions related to their work presented. NF gave advice to Sanofi-Pasteur and the World Health Organization on the efficacy profile and potential public health impact of Dengvaxia. He is also collaborating with Sanofi-Pasteur on secondary analyses of Dengvaxia clinical trial data. He has received no remuneration, grant income, expense payments or in-kind benefit from Sanofi-Pasteur. DATC and IRB have advised WHO on the use of the Sanofi vaccine in a number of meetings and as part of a consortium of modelers who estimated the potential impact of the vaccine. On occasion they received travel expenses for visits to WHO. They have also advised Sanofi Pasteur Ltd. on the implications their work has for use of their vaccine. They have not received any financial or in-kind payment from Sanofi. All other authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Gibbons R V., Kalanarooj S, Jarman RG, Nisalak A, Vaughn DW, Endy TP, et al. Analysis of repeat hospital admissions for dengue to estimate the frequency of third or fourth dengue infections resulting in admissions and dengue hemorrhagic fever, and serotype sequences. Am J Trop Med Hyg. 2007;77: 910–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical