Epidemiology and burden of multidrug-resistant bacterial infection in a developing country
- PMID: 27599374
- PMCID: PMC5030096
- DOI: 10.7554/eLife.18082
Epidemiology and burden of multidrug-resistant bacterial infection in a developing country
Abstract
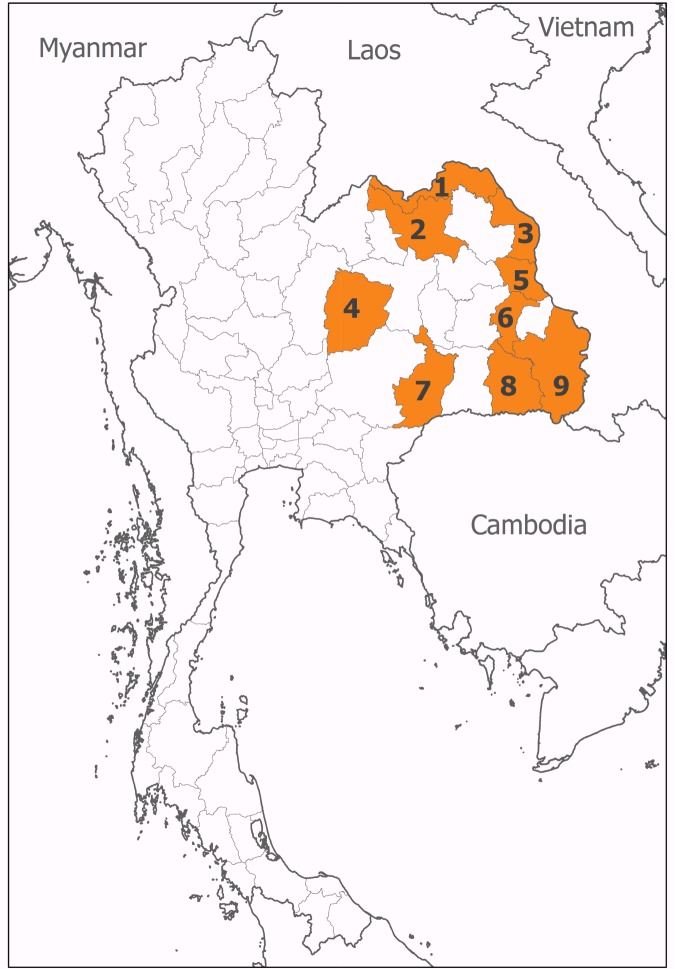
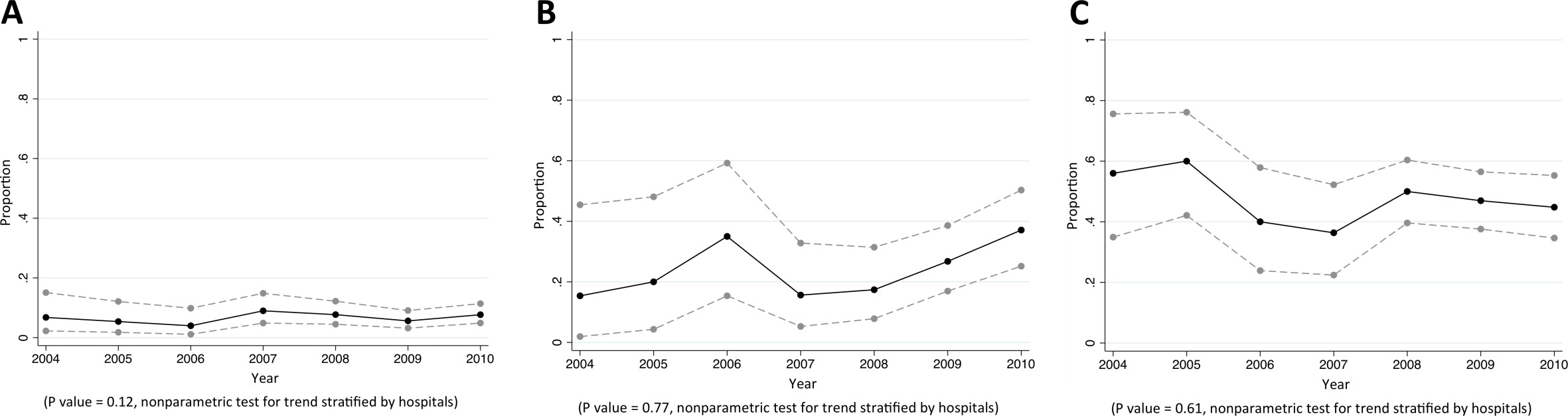
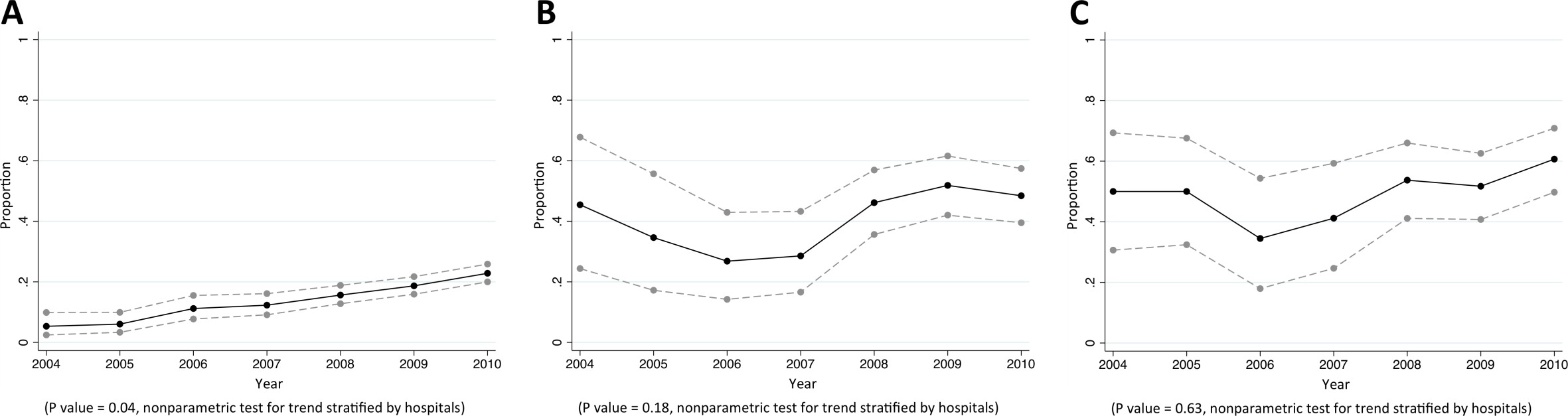
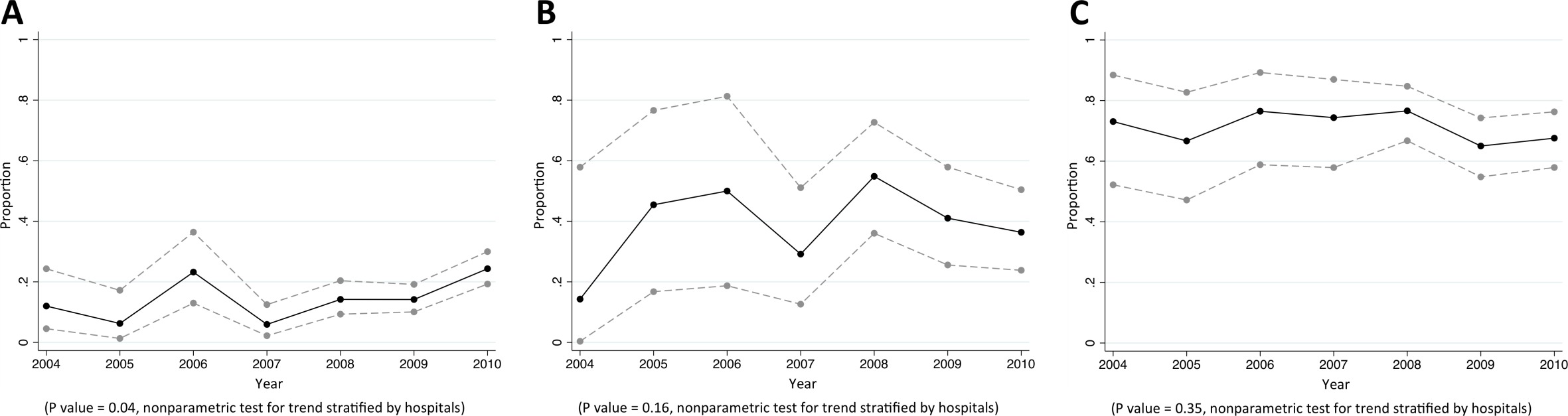
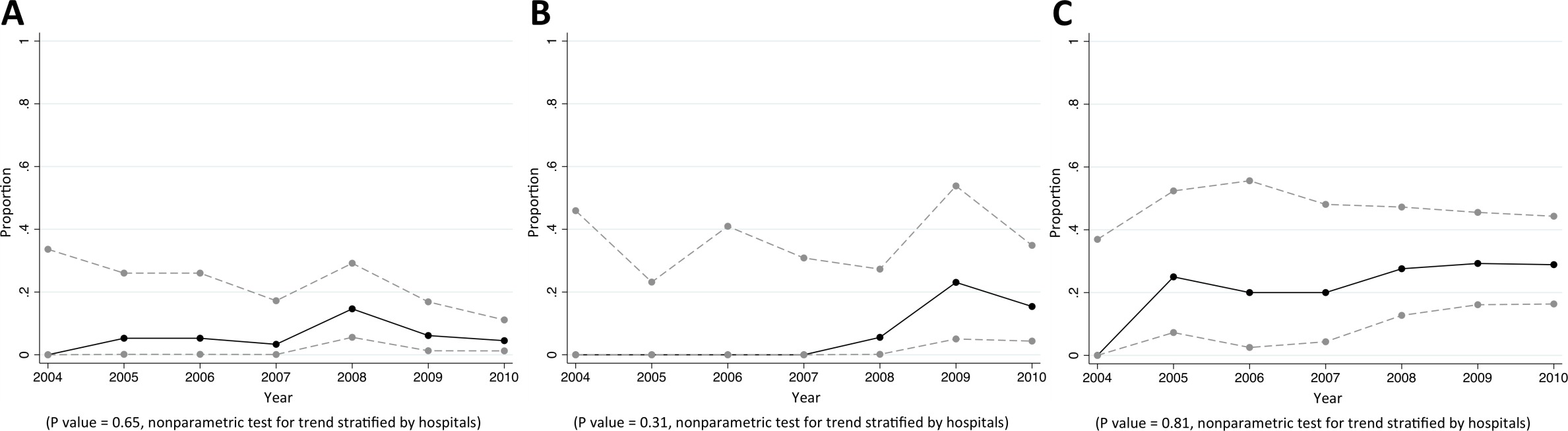
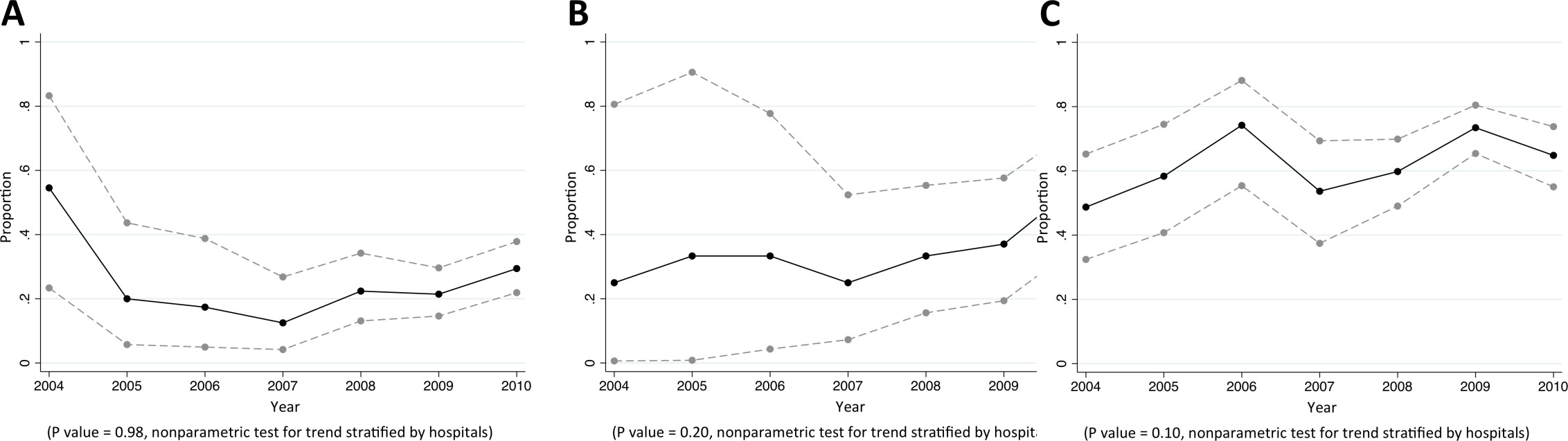
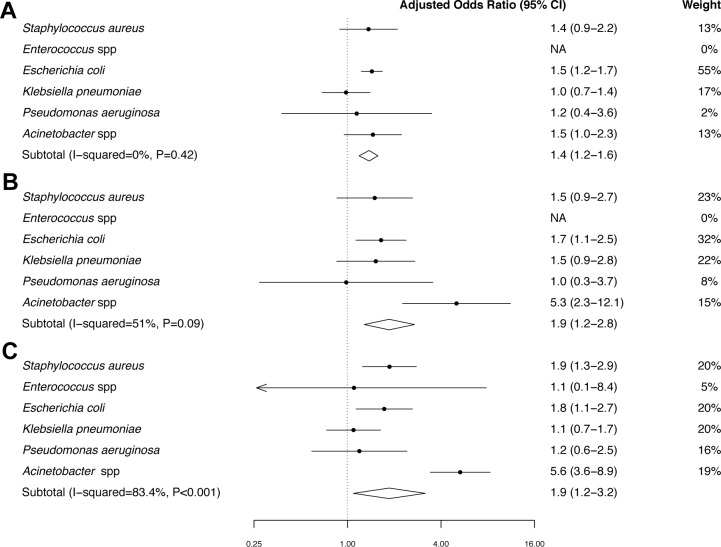
Little is known about the excess mortality caused by multidrug-resistant (MDR) bacterial infection in low- and middle-income countries (LMICs). We retrospectively obtained microbiology laboratory and hospital databases of nine public hospitals in northeast Thailand from 2004 to 2010, and linked these with the national death registry to obtain the 30-day mortality outcome. The 30-day mortality in those with MDR community-acquired bacteraemia, healthcare-associated bacteraemia, and hospital-acquired bacteraemia were 35% (549/1555), 49% (247/500), and 53% (640/1198), respectively. We estimate that 19,122 of 45,209 (43%) deaths in patients with hospital-acquired infection due to MDR bacteria in Thailand in 2010 represented excess mortality caused by MDR. We demonstrate that national statistics on the epidemiology and burden of MDR in LMICs could be improved by integrating information from readily available databases. The prevalence and mortality attributable to MDR in Thailand are high. This is likely to reflect the situation in other LMICs.
Keywords: Acinetobacter; E. coli; Enterococcus; K. pneumoniae; P. aeruginosa; Staphylococcus aureus; antimicrobial resistant; epidemiology; global health.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Ansari S, Nepal HP, Gautam R, Shrestha S, Neopane P, Gurung G, Chapagain ML. Community acquired multi-drug resistant clinical isolates of Escherichia coli in a tertiary care center of Nepal. Antimicrobial Resistance and Infection Control. 2015;4:15. doi: 10.1186/s13756-015-0059-2. - DOI - PMC - PubMed
-
- Center for Disease Controls and Prevention, U.S. Department of Health and Human Services Antibiotic resistance threats in the United States, 2013. http://www.cdc.gov/drugresistance/pdf/ar-threats-2013-508.pdf 2013
-
- Cuellar LE, Fernandez-Maldonado E, Rosenthal VD, Castaneda-Sabogal A, Rosales R, Mayorga-Espichan MJ, Camacho-Cosavalente LA, Castillo-Bravo LI. Device-associated infection rates and mortality in intensive care units of Peruvian hospitals: findings of the International Nosocomial Infection Control Consortium. Revista Panamericana De Salud Pública. 2008;24:16–24. doi: 10.1590/S1020-49892008000700002. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical