Gatifloxacin versus ceftriaxone for uncomplicated enteric fever in Nepal: an open-label, two-centre, randomised controlled trial
- PMID: 26809813
- PMCID: PMC4835582
- DOI: 10.1016/S1473-3099(15)00530-7
Gatifloxacin versus ceftriaxone for uncomplicated enteric fever in Nepal: an open-label, two-centre, randomised controlled trial
Abstract
Background: Because treatment with third-generation cephalosporins is associated with slow clinical improvement and high relapse burden for enteric fever, whereas the fluoroquinolone gatifloxacin is associated with rapid fever clearance and low relapse burden, we postulated that gatifloxacin would be superior to the cephalosporin ceftriaxone in treating enteric fever.
Methods: We did an open-label, randomised, controlled, superiority trial at two hospitals in the Kathmandu valley, Nepal. Eligible participants were children (aged 2-13 years) and adult (aged 14-45 years) with criteria for suspected enteric fever (body temperature ≥38·0°C for ≥4 days without a focus of infection). We randomly assigned eligible patients (1:1) without stratification to 7 days of either oral gatifloxacin (10 mg/kg per day) or intravenous ceftriaxone (60 mg/kg up to 2 g per day for patients aged 2-13 years, or 2 g per day for patients aged ≥14 years). The randomisation list was computer-generated using blocks of four and six. The primary outcome was a composite of treatment failure, defined as the occurrence of at least one of the following: fever clearance time of more than 7 days after treatment initiation; the need for rescue treatment on day 8; microbiological failure (ie, blood cultures positive for Salmonella enterica serotype Typhi, or Paratyphi A, B, or C) on day 8; or relapse or disease-related complications within 28 days of treatment initiation. We did the analyses in the modified intention-to-treat population, and subpopulations with either confirmed blood-culture positivity, or blood-culture negativity. The trial was powered to detect an increase of 20% in the risk of failure. This trial was registered at ClinicalTrials.gov, number NCT01421693, and is now closed.
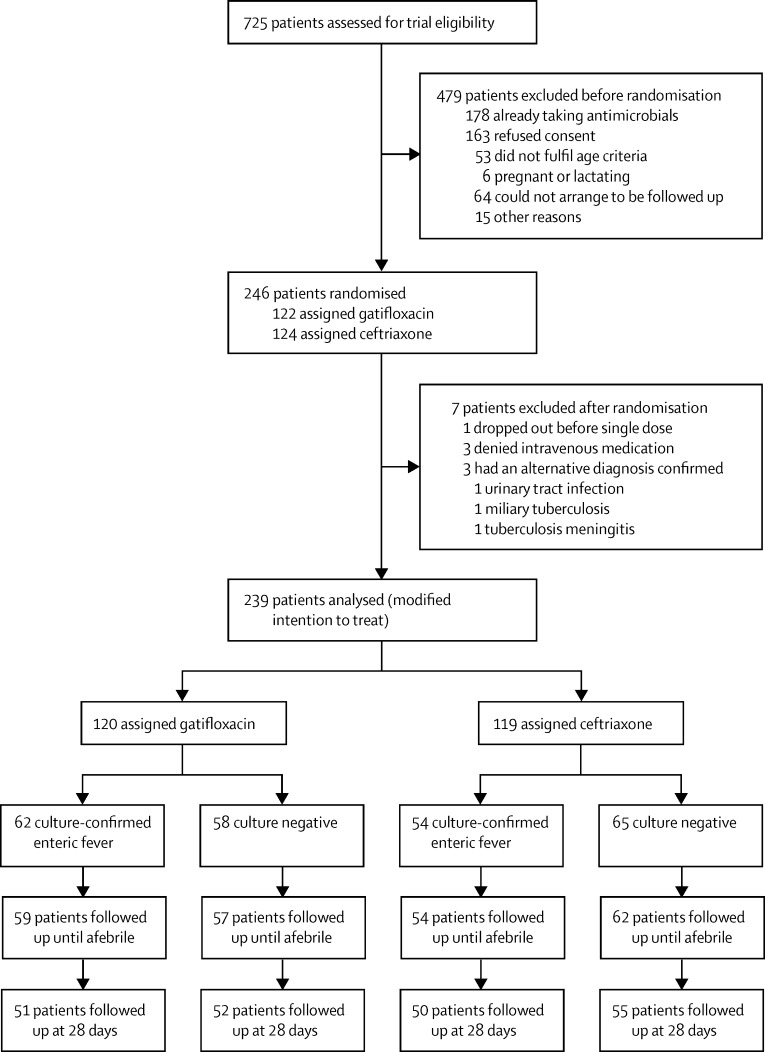
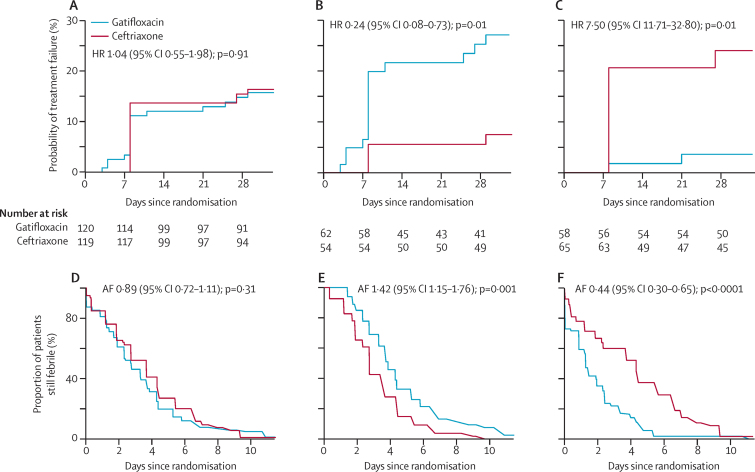
Findings: Between Sept 18, 2011, and July 14, 2014, we screened 725 patients for eligibility. On July 14, 2014, the trial was stopped early by the data safety and monitoring board because S Typhi strains with high-level resistance to ciprofloxacin and gatifloxacin had emerged. At this point, 239 were in the modified intention-to-treat population (120 assigned to gatifloxacin, 119 to ceftriaxone). 18 (15%) patients who received gatifloxacin had treatment failure, compared with 19 (16%) who received ceftriaxone (hazard ratio [HR] 1·04 [95% CI 0·55-1·98]; p=0·91). In the culture-confirmed population, 16 (26%) of 62 patients who received gatifloxacin failed treatment, compared with four (7%) of 54 who received ceftriaxone (HR 0·24 [95% CI 0·08-0·73]; p=0·01). Treatment failure was associated with the emergence of S Typhi exhibiting resistance against fluoroquinolones, requiring the trial to be stopped. By contrast, in patients with a negative blood culture, only two (3%) of 58 who received gatifloxacin failed treatment versus 15 (23%) of 65 who received ceftriaxone (HR 7·50 [95% CI 1·71-32·80]; p=0·01). A similar number of non-serious adverse events occurred in each treatment group, and no serious events were reported.
Interpretation: Our results suggest that fluoroquinolones should no longer be used for treatment of enteric fever in Nepal. Additionally, under our study conditions, ceftriaxone was suboptimum in a high proportion of patients with culture-negative enteric fever. Since antimicrobials, specifically fluoroquinolones, are one of the only routinely used control measures for enteric fever, the assessment of novel diagnostics, new treatment options, and use of existing vaccines and development of next-generation vaccines are now a high priority.
Funding: Wellcome Trust and Li Ka Shing Foundation.
Copyright © 2016 Arjyal et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
{kind=link}
{kind=link}
Comment in
-
Troubling news from Asia about treating enteric fever: a coming storm.Ryan ET. Ryan ET. Lancet Infect Dis. 2016 May;16(5):508-509. doi: 10.1016/S1473-3099(15)00542-3. Epub 2016 Jan 20. Lancet Infect Dis. 2016. PMID: 26809814 No abstract available.
-
Former first-line antibiotics for treatment of enteric fever.Gupta PK, Gupta J. Gupta PK, et al. Lancet Infect Dis. 2016 Aug;16(8):892-3. doi: 10.1016/S1473-3099(16)30143-8. Lancet Infect Dis. 2016. PMID: 27477979 No abstract available.
References
-
- Maskey AP, Basnyat B, Thwaites GE, Campbell JI, Farrar JJ, Zimmerman MD. Emerging trends in enteric fever in Nepal: 9124 cases confirmed by blood culture 1993–2003. Trans R Soc Trop Med Hyg. 2008;102:91–95. - PubMed
-
- Karkey A, Aryjal A, Basnyat B, Baker S. Kathmandu, Nepal: still an enteric fever capital of the world. J Infect Dev Ctries. 2008;2:461–465. - PubMed
-
- WHO . Background document: the diagnosis, treatment and prevention of typhoid fever. World Health Organization; Geneva: 2003. pp. 19–23.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical