FOXP3+ Regulatory T Cells in Hepatic Fibrosis and Splenomegaly Caused by Schistosoma japonicum: The Spleen May Be a Major Source of Tregs in Subjects with Splenomegaly
- PMID: 26731721
- PMCID: PMC4701139
- DOI: 10.1371/journal.pntd.0004306
FOXP3+ Regulatory T Cells in Hepatic Fibrosis and Splenomegaly Caused by Schistosoma japonicum: The Spleen May Be a Major Source of Tregs in Subjects with Splenomegaly
Erratum in
-
Correction: FOXP3+ Regulatory T Cells in Hepatic Fibrosis and Splenomegaly Caused by Schistosoma japonicum: The Spleen May Be a Major Source of Tregs in Subjects with Splenomegaly.Romano A, Hou X, Sertorio M, Dessein H, Cabantous S, Oliveira P, Li J, Oyegue S, Arnaud V, Luo X, Daujat-Chavanieu M, Mariani O, Sastre X, Dombey AM, He H, Li Y, Dessein A. Romano A, et al. PLoS Negl Trop Dis. 2016 Feb 5;10(2):e0004454. doi: 10.1371/journal.pntd.0004454. eCollection 2016 Feb. PLoS Negl Trop Dis. 2016. PMID: 26849557 Free PMC article. No abstract available.
Abstract
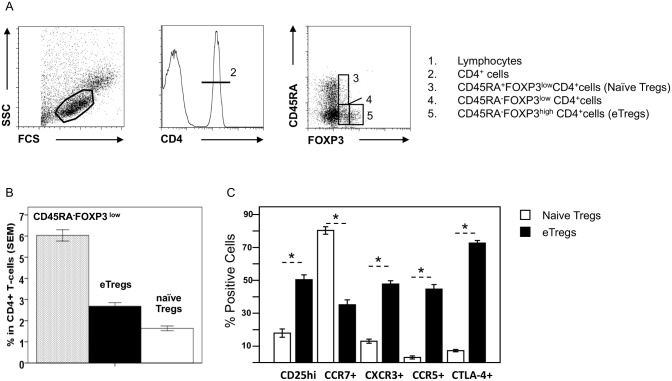
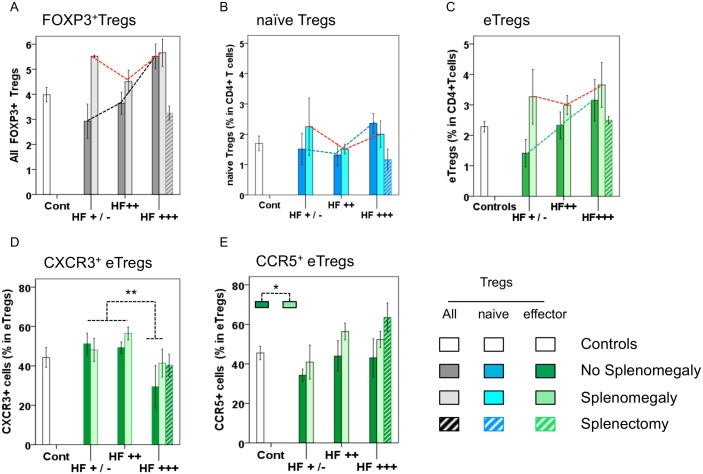
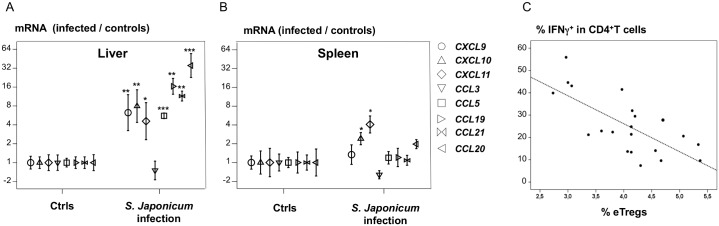
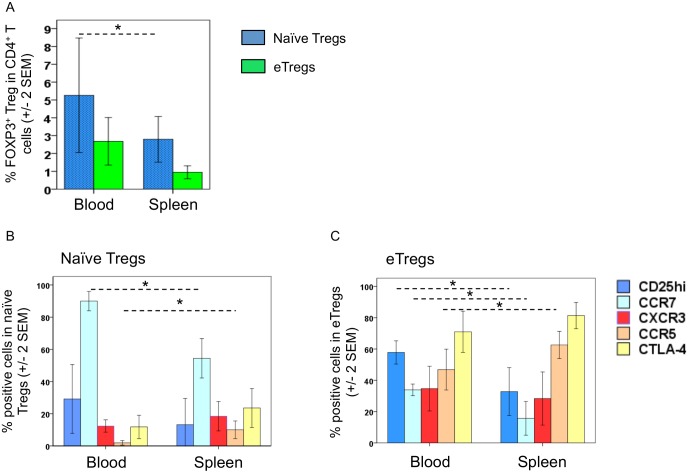
Schistosoma eggs cause chronic liver inflammation and a complex disease characterized by hepatic fibrosis (HF) and splenomegaly (SplM). FOXP3+ Tregs could regulate inflammation, but it is unclear where these cells are produced and what roles they play in human schistosomiasis. We investigated blood and spleen FOXP3+ Tregs in Chinese fishermen with lifelong exposure to Schistosoma japonicum and various degrees of liver and spleen disease. FOXP3+ Tregs accounted for 4.3% of CD4+ T cells and 41.2% of FOXP3+CD4+ T cells; they could be divided into CD45RA-FOXP3hi effector (eTregs) and CD45RA+FOXP3low naive Tregs. Blood Treg levels were high in severe HF (+1.3; p = 0.004) and in SplM (+1.03, p = 0.03). Multivariate regression showed that severe HF (+0.85, p = 0.01) and SplM (+0.97; p = 0.05) were independently associated with the higher proportion of Tregs in the blood. This effect was mostly due to an increase in the proportion of eTregs in the blood of HF+++ (+0.9%; p = 0.04) and SplM (+0.9%; p = 0.04) patients. The proportion of eTregs expressing CXCR3 in the blood was lower in the HF+++ patients (37.4 +/- 5.9%) than in those with milder fibrosis (51.7 ± 2%; p = 0.009), whereas proportion were similar for cells expressing CD25hi, CCR7, and CTLA-4. Splenectomy improves symptoms and was associated with decreases in blood FOXP3+ Treg (-2.5; p<0.001) and eTreg (-1.3; p = 0.03) levels. SplM spleens contained a high proportion of eTregs with CXCR3, CCR5 and CTLA4 upregulation and CCR7 downregulation. This, and the strong expression of ligands of CXCR3 and CCR5 in the liver (n = 8) but not in the spleen suggested that spleen eTregs migrated to Th1-infiltrated liver tissues. Such migration may be attenuated in hepatosplenic patients due to lower levels of CXCR3 expression on Tregs (p = 0.009). Thus, higher blood Treg levels are associated with severe liver disease and splenomegaly. Our data are consistent with the hypothesis that the spleen is a major source of Tregs in subjects with splenomegaly. In most cases, Tregs migrate to the Th1-infiltrated liver and the lower levels of CXCR3+ Tregs in the blood of patients with severe schistosomiasis suggest that decreases in Treg migration sites of inflammation may aggravate the disease.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Fontenot JD, Gavin MA, Rudensky AY. Foxp3 programs the development and function of CD4+CD25+ regulatory T cells. Nature immunology. 2003;4(4):330–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous