Estimating the Future Impact of a Multi-Pronged Intervention Strategy on Ocular Disease Sequelae Caused by Trachoma: A Modeling Study
- PMID: 26653262
- PMCID: PMC4841017
- DOI: 10.3109/09286586.2015.1081249
Estimating the Future Impact of a Multi-Pronged Intervention Strategy on Ocular Disease Sequelae Caused by Trachoma: A Modeling Study
Abstract
Purpose: Trachoma control programs are underway in endemic regions worldwide. They are based on the SAFE strategy (Surgery for trichiasis, Antibiotic distribution, Facial cleanliness, and Environmental improvement). Although much is known about the effect of community-wide treatment with antibiotics on the prevalence of Chlamydia trachomatis, the impact of the SAFE strategy on severe ocular disease sequelae (the main focus of the Global Elimination of blinding Trachoma by 2020 program) remains largely unknown.
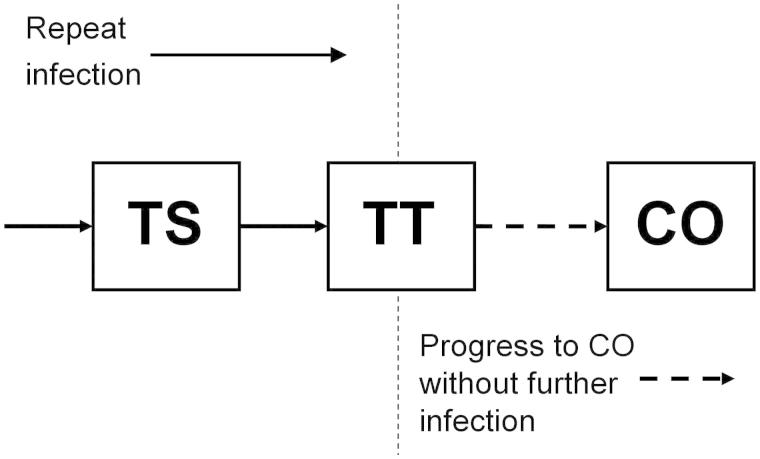
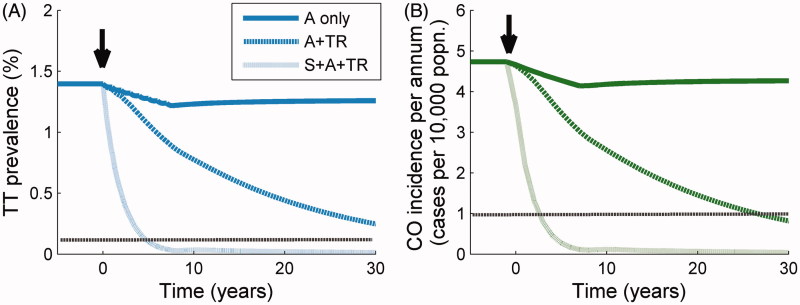
Methods: We use a mathematical model to explore the impact of each of the components of the SAFE strategy, individually and together, on disease sequelae, arising from repeat infection and subsequent conjunctival scarring. We ask whether two elimination goals, to reduce the prevalence of trachomatous trichiasis to 1 per 1000 persons, and the incidence of corneal opacity to 1 per 10,000 persons per annum, are achievable, and which combinations of interventions have the greatest impact on these indicators.
Results: In high prevalence communities (here, >20% infection of children aged 1-9 years), a combination of efforts is needed to bring down sustainably the prevalence and incidence of ocular disease sequelae.
Conclusion: The mass delivery of antibiotics is highly beneficial for the clearance of infection, inflammation and prevention of subsequent scarring, but needs to be supplemented with sustained reductions in transmission and surgery to consider realistically the elimination of blindness by the year 2020.
Keywords: Blindness; Chlamydia trachomatis; elimination program; mathematical modeling; ocular sequelae.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- WHO. Prevention of blindness and visual impairment: Trachoma. 2009. Accessed June 25, 2009 from: http://www.who.int/blindness/causes/trachoma/en/index.html
-
- Kuper H, Solomon AW, Buchan J, et al. A critical review of the SAFE strategy for the prevention of blinding trachoma. Lancet Infect Dis. 2003;3:372–381. - PubMed
-
- Mariotti SP, Pascolini D, Rose-Nussbaumer J. Trachoma: global magnitude of a preventable cause of blindness. Br J Ophthalmol. 2009;93:563–568. - PubMed
-
- Taylor HR. Trachoma grading: a new grading scheme. Rev Int Trach Pathol Ocul Trop Subtrop Sante Publique. 1987;(64):175–181. - PubMed
-
- ITI Frequently Asked Questions. 2012. Accessed June 5, 2012 from: http://trachoma.org/iti-frequently-asked-questions
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources