Estimating distributions of health state severity for the global burden of disease study
- PMID: 26582970
- PMCID: PMC4650517
- DOI: 10.1186/s12963-015-0064-y
Estimating distributions of health state severity for the global burden of disease study
Abstract
Background: Many major causes of disability in the Global Burden of Disease (GBD) study present with a range of severity, and for most causes finding population distributions of severity can be difficult due to issues of sparse data, inconsistent measurement, and need to account for comorbidities. We developed an indirect approach to obtain severity distributions empirically from survey data.
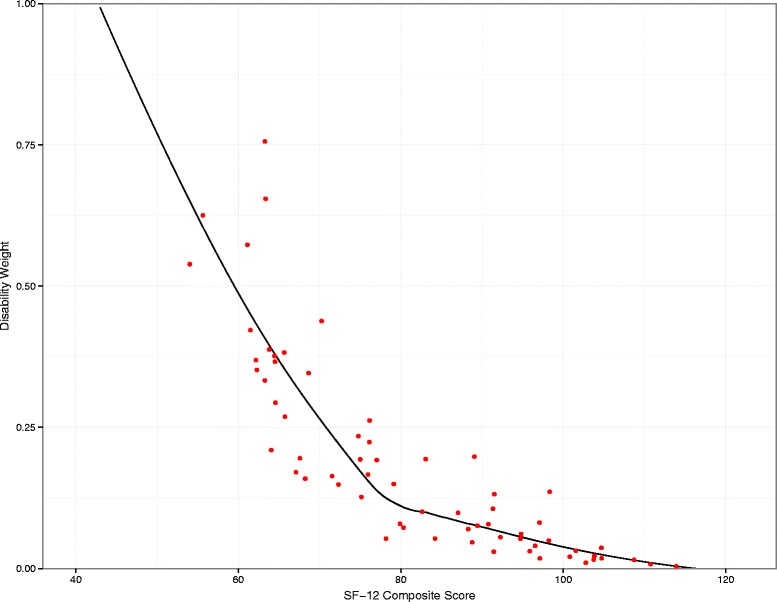
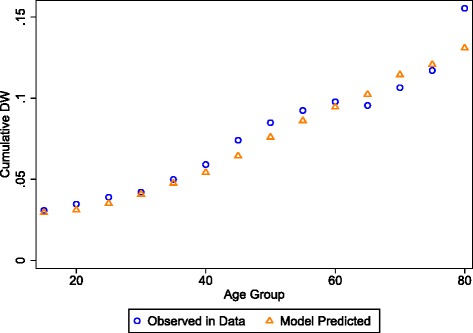
Methods: Individual-level data were used from three large population surveys from the US and Australia that included self-reported prevalence of major diseases and injuries as well as generic health status assessments using the 12-Item Short Form Health Survey (SF-12). We developed a mapping function from SF-12 scores to GBD disability weights. Mapped scores for each individual respondent were regressed against the reported diseases and injuries using a mixed-effects model with a logit-transformed response variable. The regression outputs were used to predict comorbidity-corrected health-state weights for the group of individuals with each condition. The distribution of these comorbidity-corrected weights were used to estimate the fraction of individuals with each condition falling into different GBD severity categories, including asymptomatic (implying disability weight of zero).
Results: After correcting for comorbid conditions, all causes analyzed had some proportion of the population in the asymptomatic category. For less severe conditions, such as alopecia areata, we estimated that 44.1 % [95 % CI: 38.7 %-49.4 %] were asymptomatic while 28.3 % [26.8 %-29.6 %] of anxiety disorders had asymptomatic cases. For 152 conditions, full distributions of severity were estimated. For anxiety disorders for example, we estimated the mean population proportions in the mild, moderate, and severe states to be 40.9 %, 18.5 %, and 12.3 % respectively. Thirty-seven of the analyzed conditions were used in the GBD 2013 estimates and are reported here.
Conclusion: There is large heterogeneity in the disabling severity of conditions among individuals. The GBD 2013 approach allows explicit accounting for this heterogeneity in GBD estimates. Existing survey data that have collected health status together with information on the presence of a series of comorbid conditions can be used to fill critical gaps in the information on condition severity while correcting for effects of comorbidity. Our ability to make these estimates may be limited by lack of geographic variation in the data and by the current methodology for disability weights, which implies that severity must be binned rather than expressed in as a full distribution. Future country-specific data collection efforts will be needed to advance this research.
Keywords: 12-item short form health survey (SF-12); Disability weights; Functional health status; Global burden of disease; Medical expenditures panel survey (MEPS); Non-fatal outcomes.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2163–2196. doi: 10.1016/S0140-6736(12)61729-2. - DOI - PMC - PubMed
-
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2197–2223. doi: 10.1016/S0140-6736(12)61689-4. - DOI - PubMed
-
- Salomon JA, Wang H, Freeman MK, Vos T, Flaxman AD, Lopez AD, et al. Healthy life expectancy for 187 countries, 1990–2010: a systematic analysis for the Global Burden Disease Study 2010. Lancet. 2012;2012(380):2144–62. - PubMed
-
- Salomon JA, Vos T, Hogan DR, Gagnon M, Naghavi M, Mokdad A, et al. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet. 2012;380:2129–2143. doi: 10.1016/S0140-6736(12)61680-8. - DOI - PMC - PubMed
-
- Salomon JA, Mathers CD, Chatterji S, Sadana R, Ustun TB, Murray CJL. Chapter 26: Quantifying Individual Levels of Health: Definitions, Concepts, and Measurement Issues. In: Health systems performance assessment: debates, methods and empiricism. Geneva: World Health Organization; 2003.
LinkOut - more resources
Full Text Sources
Other Literature Sources