Public health impact and cost-effectiveness of the RTS,S/AS01 malaria vaccine: a systematic comparison of predictions from four mathematical models
- PMID: 26549466
- PMCID: PMC4723722
- DOI: 10.1016/S0140-6736(15)00725-4
Public health impact and cost-effectiveness of the RTS,S/AS01 malaria vaccine: a systematic comparison of predictions from four mathematical models
Abstract
Background: The phase 3 trial of the RTS,S/AS01 malaria vaccine candidate showed modest efficacy of the vaccine against Plasmodium falciparum malaria, but was not powered to assess mortality endpoints. Impact projections and cost-effectiveness estimates for longer timeframes than the trial follow-up and across a range of settings are needed to inform policy recommendations. We aimed to assess the public health impact and cost-effectiveness of routine use of the RTS,S/AS01 vaccine in African settings.
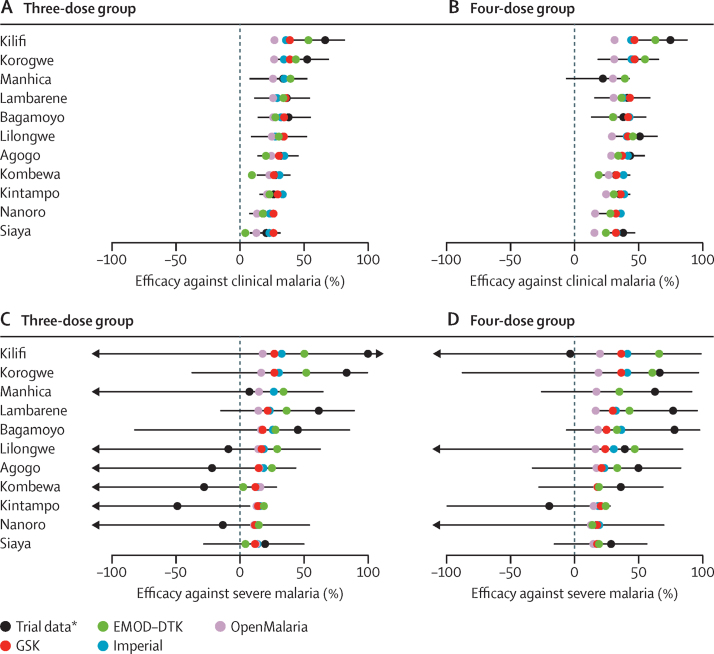
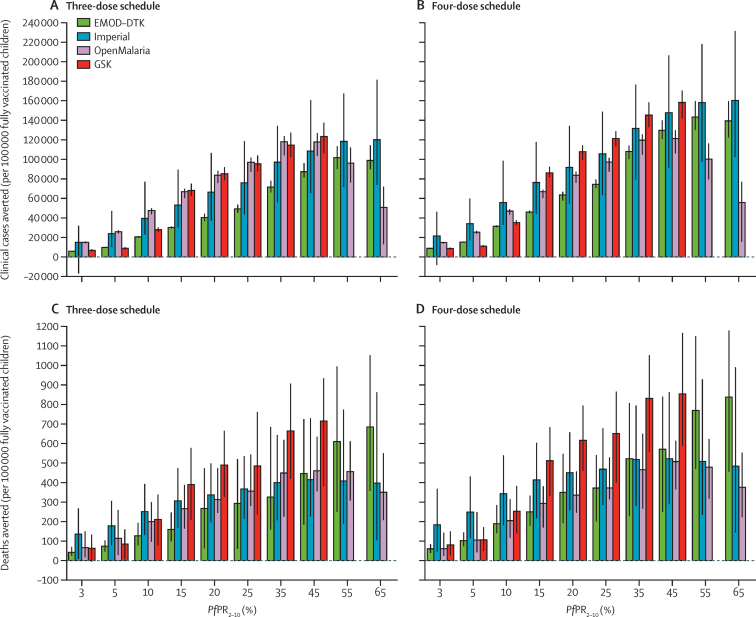
Methods: We compared four malaria transmission models and their predictions to assess vaccine cost-effectiveness and impact. We used trial data for follow-up of 32 months or longer to parameterise vaccine protection in the group aged 5-17 months. Estimates of cases, deaths, and disability-adjusted life-years (DALYs) averted were calculated over a 15 year time horizon for a range of levels of Plasmodium falciparum parasite prevalence in 2-10 year olds (PfPR2-10; range 3-65%). We considered two vaccine schedules: three doses at ages 6, 7·5, and 9 months (three-dose schedule, 90% coverage) and including a fourth dose at age 27 months (four-dose schedule, 72% coverage). We estimated cost-effectiveness in the presence of existing malaria interventions for vaccine prices of US2ドル-10 per dose.
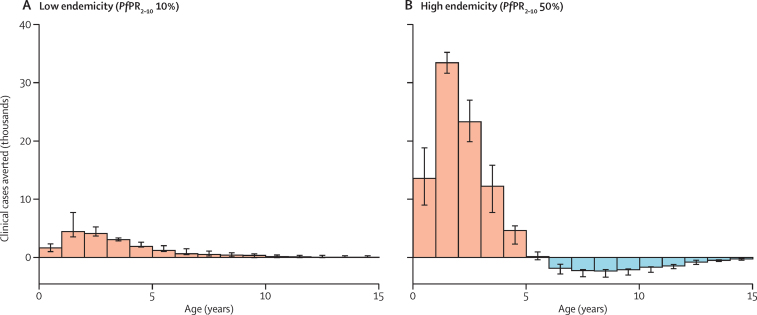
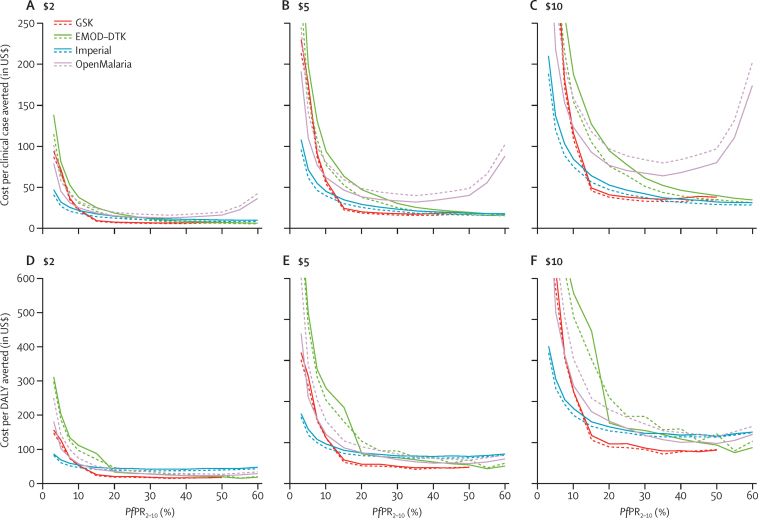
Findings: In regions with a PfPR2-10 of 10-65%, RTS,S/AS01 is predicted to avert a median of 93,940 (range 20,490-126,540) clinical cases and 394 (127-708) deaths for the three-dose schedule, or 116,480 (31,450-160,410) clinical cases and 484 (189-859) deaths for the four-dose schedule, per 100,000 fully vaccinated children. A positive impact is also predicted at a PfPR2-10 of 5-10%, but there is little impact at a prevalence of lower than 3%. At 5ドル per dose and a PfPR2-10 of 10-65%, we estimated a median incremental cost-effectiveness ratio compared with current interventions of 30ドル (range 18-211) per clinical case averted and 80ドル (44-279) per DALY averted for the three-dose schedule, and of 25ドル (16-222) and 87ドル (48-244), respectively, for the four-dose schedule. Higher ICERs were estimated at low PfPR2-10 levels.
Interpretation: We predict a significant public health impact and high cost-effectiveness of the RTS,S/AS01 vaccine across a wide range of settings. Decisions about implementation will need to consider levels of malaria burden, the cost-effectiveness and coverage of other malaria interventions, health priorities, financing, and the capacity of the health system to deliver the vaccine.
Funding: PATH Malaria Vaccine Initiative; Bill & Melinda Gates Foundation; Global Good Fund; Medical Research Council; UK Department for International Development; GAVI, the Vaccine Alliance; WHO.
Copyright © 2016 Penny et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comment in
-
Implementation of the malaria candidate vaccine RTS,S/AS01.Greenwood B, Doumbo OK. Greenwood B, et al. Lancet. 2016 Jan 23;387(10016):318-319. doi: 10.1016/S0140-6736(15)00807-7. Epub 2015 Nov 6. Lancet. 2016. PMID: 26549465 No abstract available.
References
-
- WHO . World malaria report 2013. World Health Organization; Geneva: 2014.
-
- Hamel MJ, Oneko M, Williamson J. A marked reduction in mortality among participants in a clinical trial that removed barriers to care and implemented national case management guidelines. 63rd Annual meeting of the American Society of Tropical Medicine and Hygiene; New Orleans, LA; Nov 2–6, 2014. 631 (abstr).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical