The time-course of protection of the RTS,S vaccine against malaria infections and clinical disease
- PMID: 26537608
- PMCID: PMC4634589
- DOI: 10.1186/s12936-015-0969-8
The time-course of protection of the RTS,S vaccine against malaria infections and clinical disease
Abstract
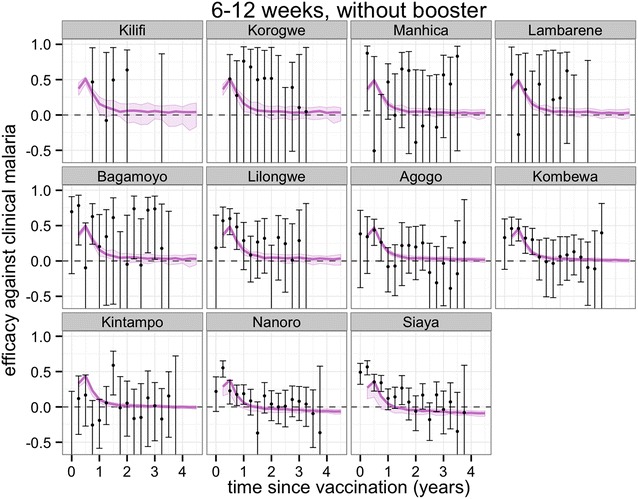
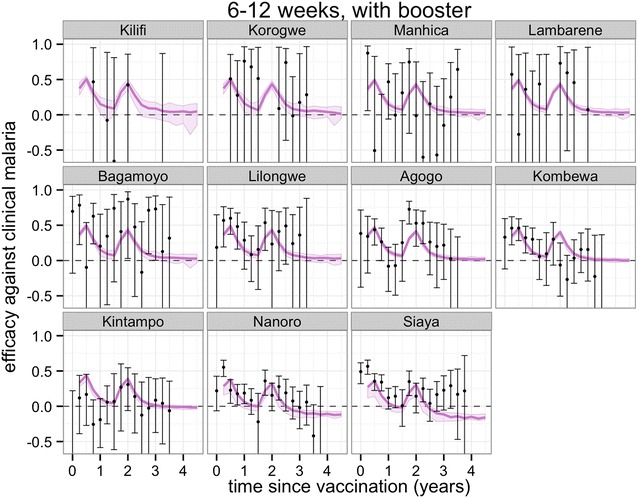
Background: Recent publications have reported follow-up of the RTS,S/AS01 malaria vaccine candidate Phase III trials at 11 African sites for 32 months (or longer). This includes site- and time-specific estimates of incidence and efficacy against clinical disease with four different vaccination schedules. These data allow estimation of the time-course of protection against infection associated with two different ages of vaccination, both with and without a booster dose.
Methods: Using an ensemble of individual-based stochastic models, each trial cohort in the Phase III trial was simulated assuming many different hypothetical profiles for the vaccine efficacy against infection in time, for both the primary course and boosting dose and including the potential for either exponential or non-exponential decay. The underlying profile of protection was determined by Bayesian fitting of these model predictions to the site- and time-specific incidence of clinical malaria over 32 months (or longer) of follow-up. Using the same stochastic models, projections of clinical efficacy in each of the sites were modelled and compared to available observed trial data.
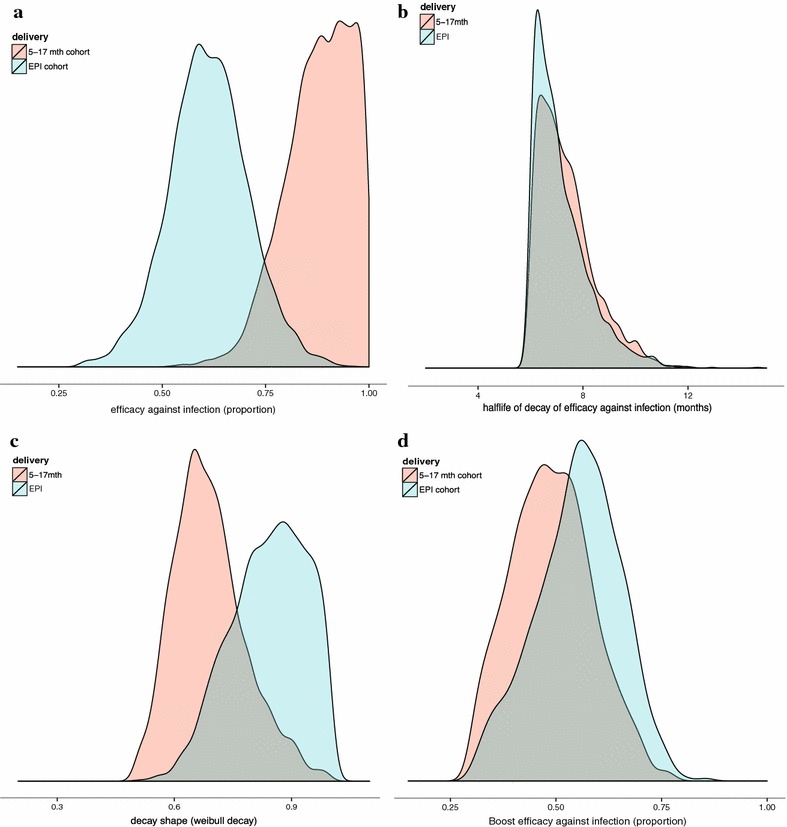
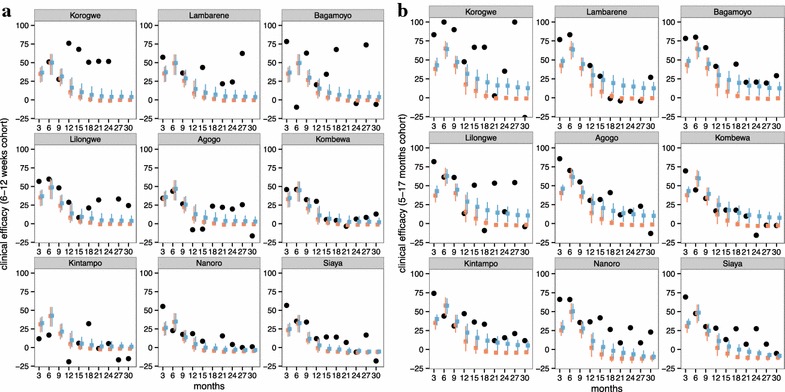
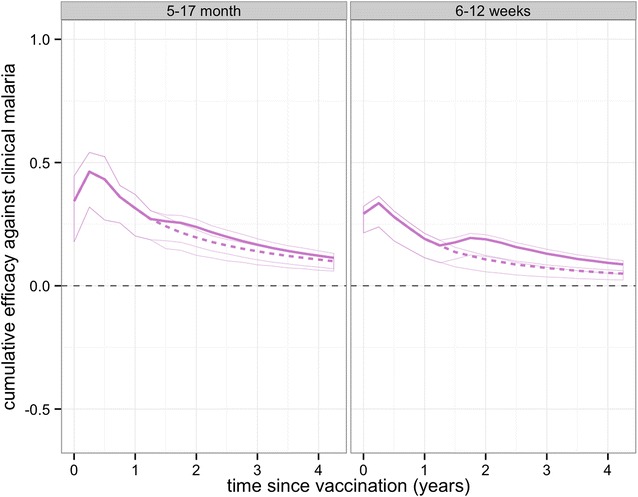
Results: The initial protection of RTS,S immediately following three doses is estimated as providing an efficacy against infection of 65 % (when immunizing infants aged 6-12 weeks old) and 91 % (immunizing children aged 5-17 months old at first vaccination). This protection decays relatively rapidly, with an approximately exponential decay for the 6-12 weeks old cohort (with a half-life of 7.2 months); for the 5-17 months old cohort a biphasic decay with a similar half-life is predicted, with an initial rapid decay followed by a slower decay. The boosting dose was estimated to return protection to an efficacy against infection of 50-55 % for both cohorts. Estimates of clinical efficacy by trial site are consistent with those reported in the trial for all cohorts.
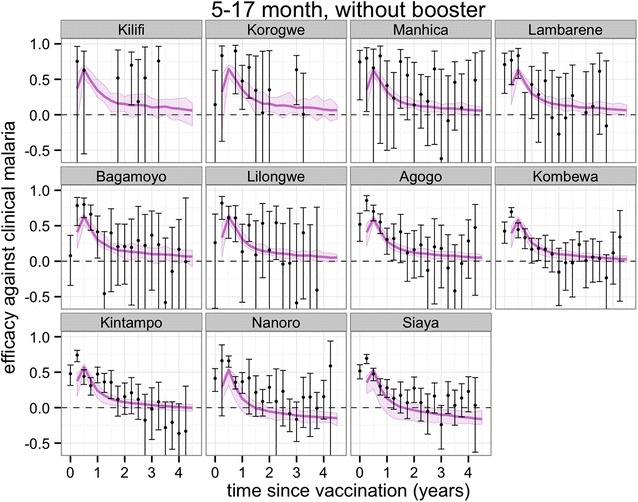
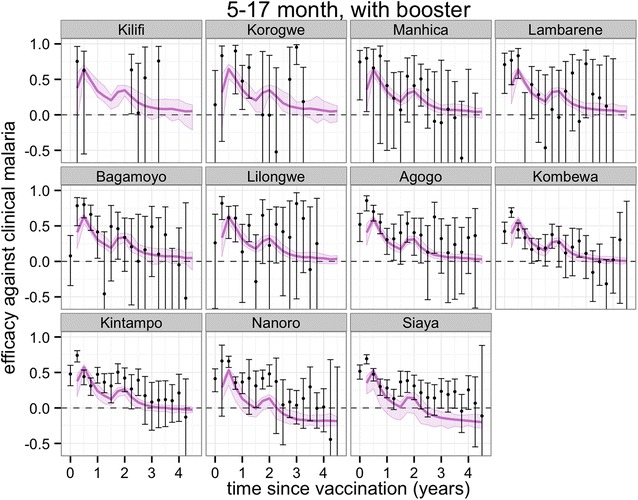
Conclusions: The site- and time-specific clinical observations from the RTS,S/AS01 trial data allowed a reasonably precise estimation of the underlying vaccine protection against infection which is consistent with common underlying efficacy and decay rates across the trial sites. This calibration suggests that the decay in efficacy against clinical disease is more rapid than that against infection because of age-shifts in the incidence of disease. The dynamical models predict that clinical effectiveness will continue to decay and that likely effects beyond the time-scale of the trial will be small.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- World Health Organization . World Malaria Report 2013. Geneva: World Health Organization; 2014.
-
- RTSS Clinical Trials Partnership Efficacy and safety of RTS,S/AS01 malaria vaccine with or without a booster dose in infants and children in Africa: final results of a phase 3, individually randomised, controlled trial. Lancet. 2015;386:31–45. doi: 10.1016/S0140-6736(15)60721-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical