Toxicity of Amphotericin B Deoxycholate-Based Induction Therapy in Patients with HIV-Associated Cryptococcal Meningitis
- PMID: 26349818
- PMCID: PMC4649151
- DOI: 10.1128/AAC.01698-15
Toxicity of Amphotericin B Deoxycholate-Based Induction Therapy in Patients with HIV-Associated Cryptococcal Meningitis
Abstract
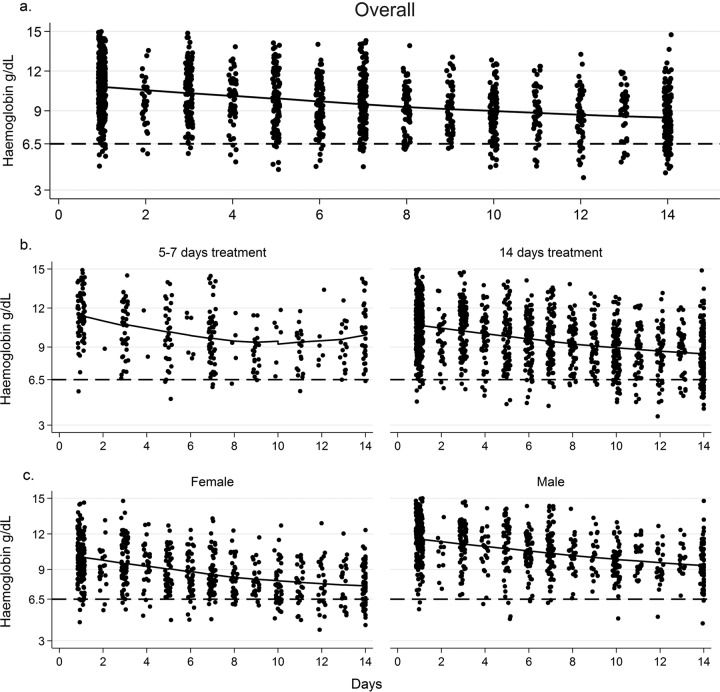
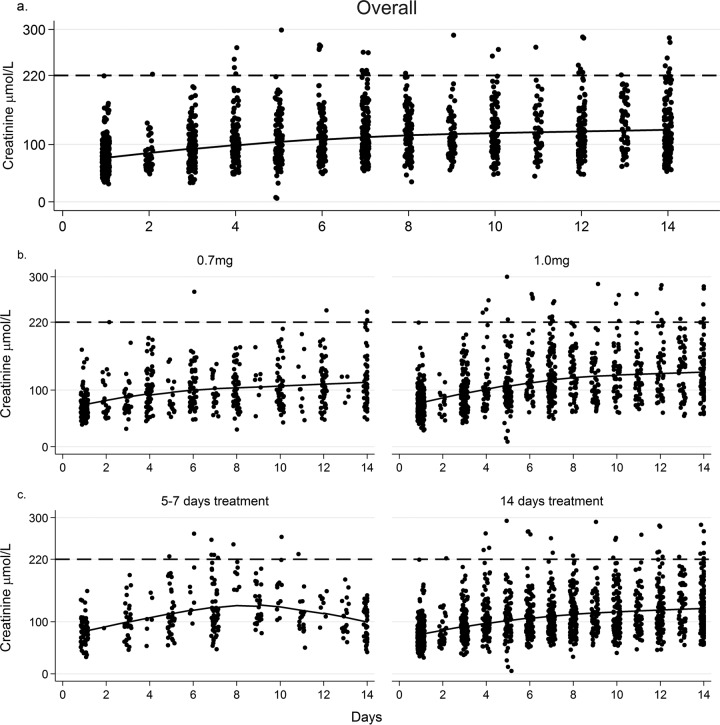
Amphotericin B deoxycholate (AmBd) is the recommended induction treatment for HIV-associated cryptococcal meningitis (CM). Its use is hampered by toxicities that include electrolyte abnormalities, nephrotoxicity, and anemia. Protocols to minimize toxicity are applied inconsistently. In a clinical trial cohort of AmBd-based CM induction treatment, a standardized protocol of preemptive hydration and electrolyte supplementation was applied. Changes in blood counts, electrolyte levels, and creatinine levels over 14 days were analyzed in relation to the AmBd dose, treatment duration (short course of 5 to 7 days or standard course of 14 days), addition of flucytosine (5FC), and outcome. In the 368 patients studied, the hemoglobin levels dropped by a mean of 1.5 g/dl (95% confidence interval [CI], 1.0 to 1.9 g/dl) following 7 days of AmBd and by a mean of 2.3 g/dl (95% CI, 1.1 to 3.6 g/dl) after 14 days. Serum creatinine levels increased by 37 μmol/liter (95% CI, 30 to 45 μmol/liter) by day 7 and by 49 μmol/liter (95% CI, 35 to 64μmol/liter) by day 14 of AmBd treatment. Overall, 33% of patients developed grade III/IV anemia, 5.6% developed grade III hypokalemia, 9.5% had creatinine levels that exceeded 220 μmol, and 6% discontinued AmBd prematurely. The addition of 5FC was associated with a slight increase in anemia but not neutropenia. Laboratory abnormalities stabilized or reversed during the second week in patients on short-course induction. Grade III/IV anemia (adjusted odds ratio [aOR], 2.2; 95% CI, 1.1 to 4.3; P = 0.028) and nephrotoxicity (aOR, 4.5; 95% CI, 1.8 to 11; P = 0.001) were risk factors for 10-week mortality. In summary, routine intravenous saline hydration and preemptive electrolyte replacement during AmBd-based induction regimens for HIV-associated CM minimized the incidence of hypokalemia and nephrotoxicity. Anemia remained a concerning adverse effect. The addition of flucytosine was not associated with increased neutropenia. Shorter AmBd courses were less toxic, with rapid reversibility.
Copyright © 2015 Bicanic et al.
Figures
{kind=link}
{kind=link}
References
-
- Dismukes WE, Cloud G, Gallis HA, Kerkering TM, Medoff G, Craven PC, Kaplowitz LG, Fisher JF, Gregg CR, Bowles CA. 1987. Treatment of cryptococcal meningitis with combination amphotericin B and flucytosine for four as compared with six weeks. N Engl J Med 317:334–341. doi:10.1056/NEJM198708063170602. - DOI - PubMed
-
- Bennett JE, Dismukes WE, Duma RJ, Medoff G, Sande MA, Gallis H, Leonard J, Fields BT, Bradshaw M, Haywood H. 1979. A comparison of amphotericin B alone and combined with flucytosine in the treatment of cryptoccal [sic] meningitis. N Engl J Med 301:126–131. doi:10.1056/NEJM197907193010303. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical