Peripheral opioid antagonist enhances the effect of anti-tumor drug by blocking a cell growth-suppressive pathway in vivo
- PMID: 25853862
- PMCID: PMC4390307
- DOI: 10.1371/journal.pone.0123407
Peripheral opioid antagonist enhances the effect of anti-tumor drug by blocking a cell growth-suppressive pathway in vivo
Abstract
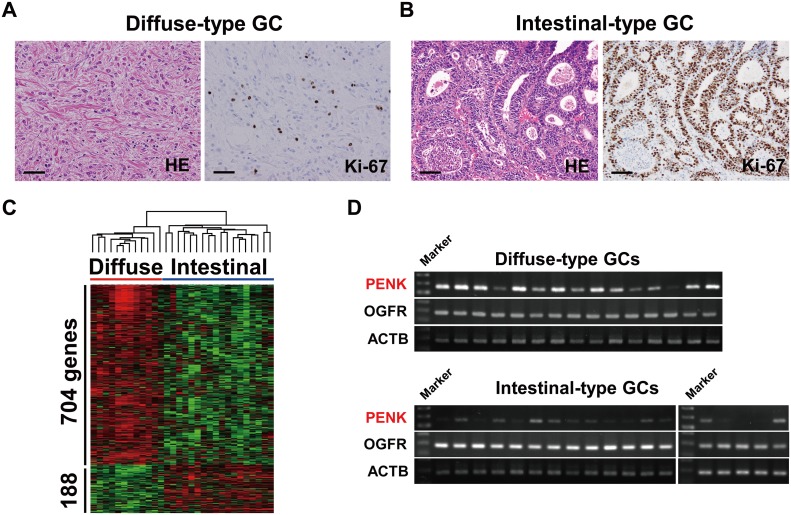
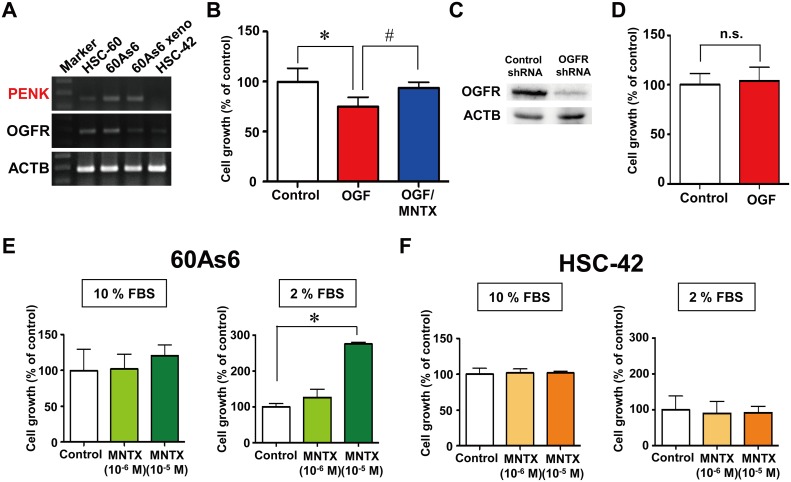
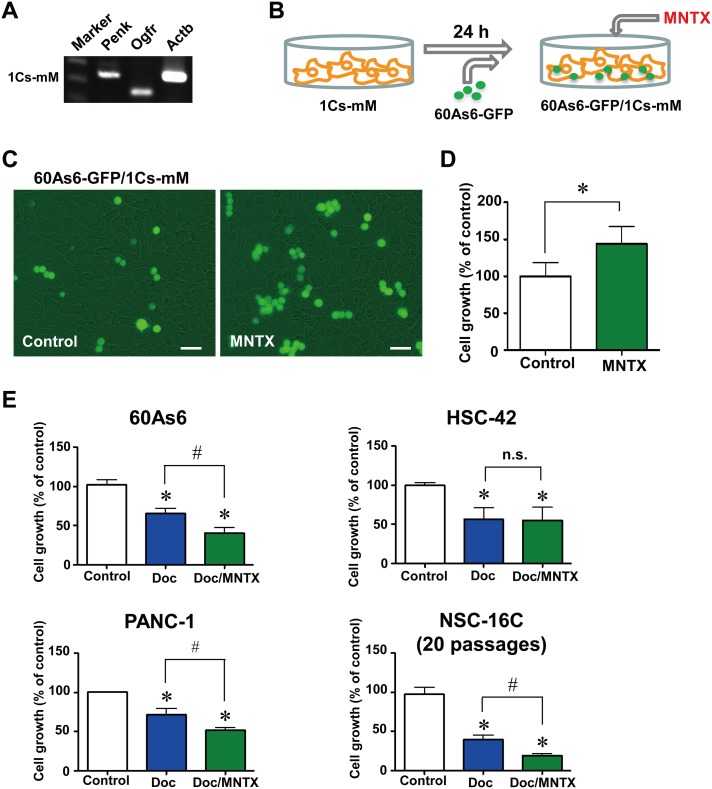
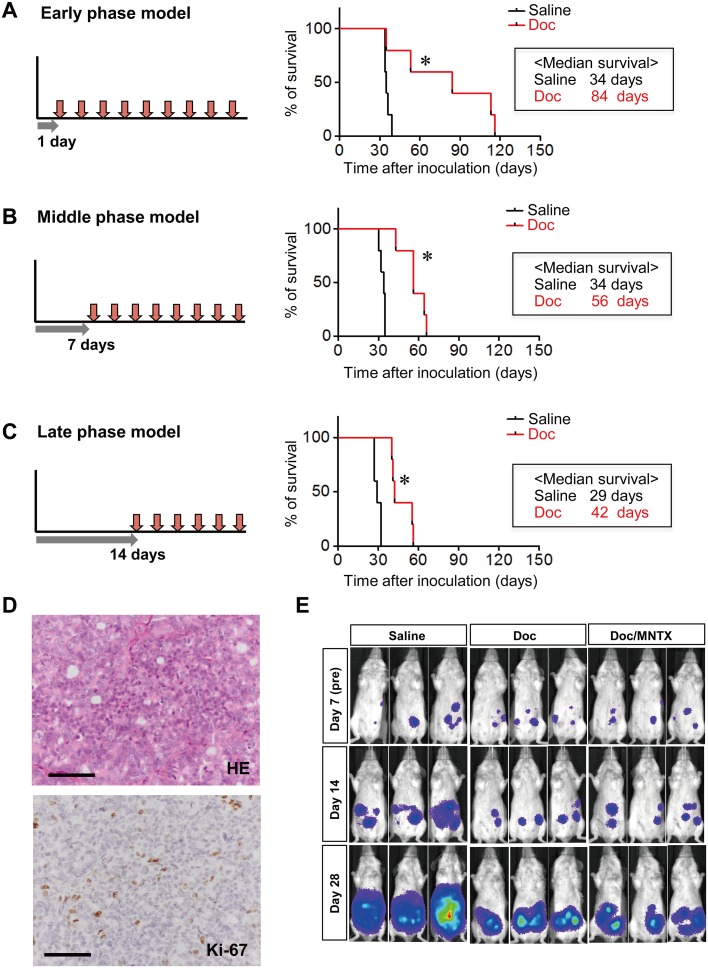
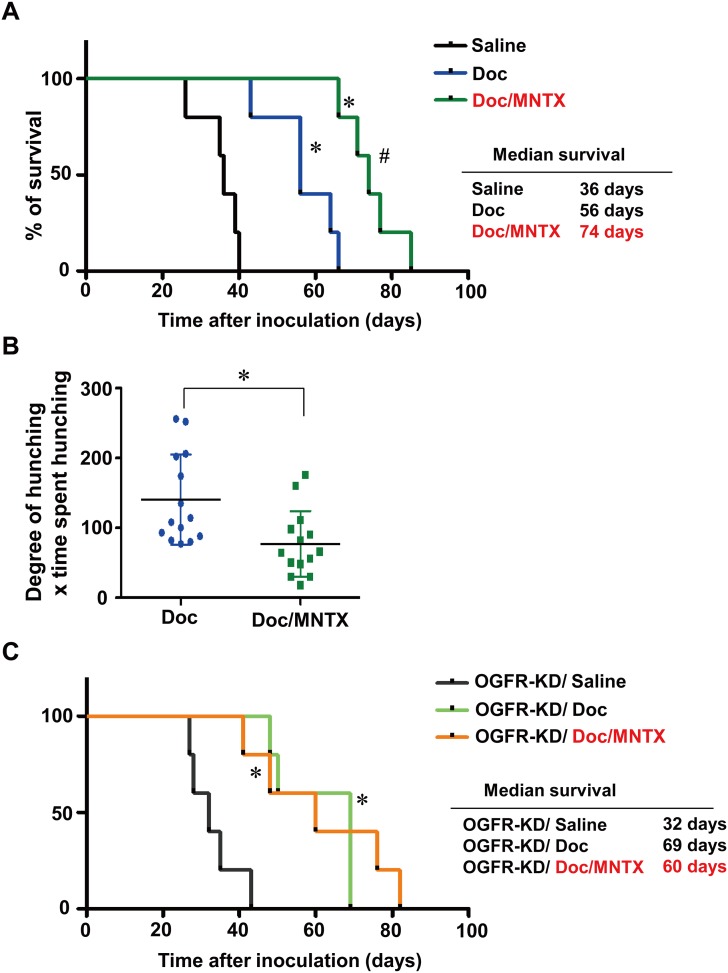
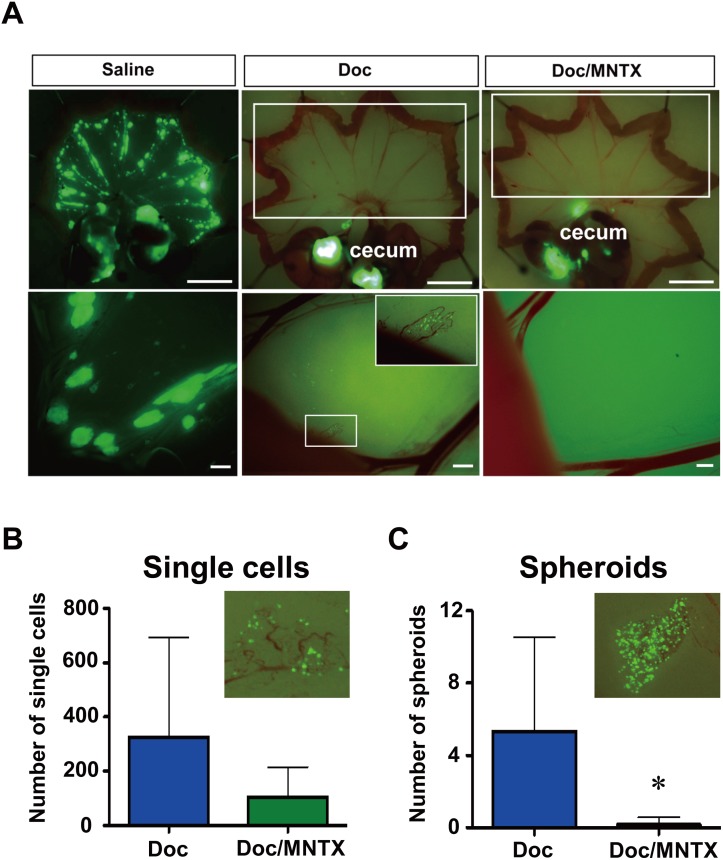
The dormancy of tumor cells is a major problem in chemotherapy, since it limits the therapeutic efficacy of anti-tumor drugs that only target dividing cells. One potential way to overcome chemo-resistance is to "wake up" these dormant cells. Here we show that the opioid antagonist methylnaltrexone (MNTX) enhances the effect of docetaxel (Doc) by blocking a cell growth-suppressive pathway. We found that PENK, which encodes opioid growth factor (OGF) and suppresses cell growth, is predominantly expressed in diffuse-type gastric cancers (GCs). The blockade of OGF signaling by MNTX releases cells from their arrest and boosts the effect of Doc. In comparison with the use of Doc alone, the combined use of Doc and MNTX significantly prolongs survival, alleviates abdominal pain, and diminishes Doc-resistant spheroids on the peritoneal membrane in model mice. These results suggest that blockade of the pathways that suppress cell growth may enhance the effects of anti-tumor drugs.
Conflict of interest statement
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. An attempt at a histo-clinical classification. Acta Pathol. Microbiol. Scand. 1965;64: 31–49. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous