Mycetoma in the Sudan: an update from the Mycetoma Research Centre, University of Khartoum, Sudan
- PMID: 25816316
- PMCID: PMC4376889
- DOI: 10.1371/journal.pntd.0003679
Mycetoma in the Sudan: an update from the Mycetoma Research Centre, University of Khartoum, Sudan
Abstract
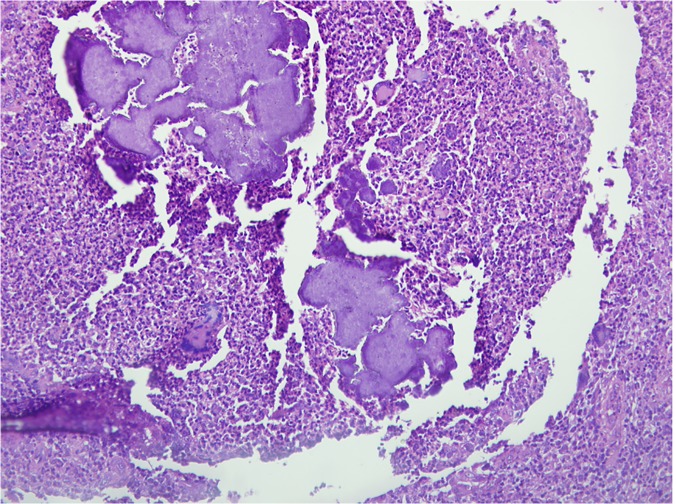
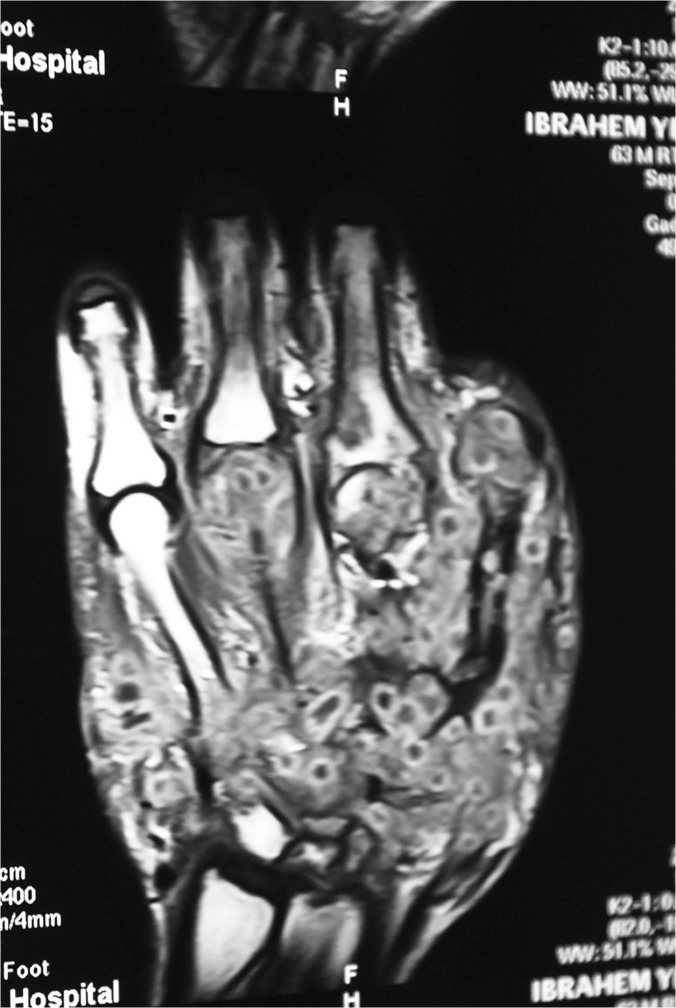
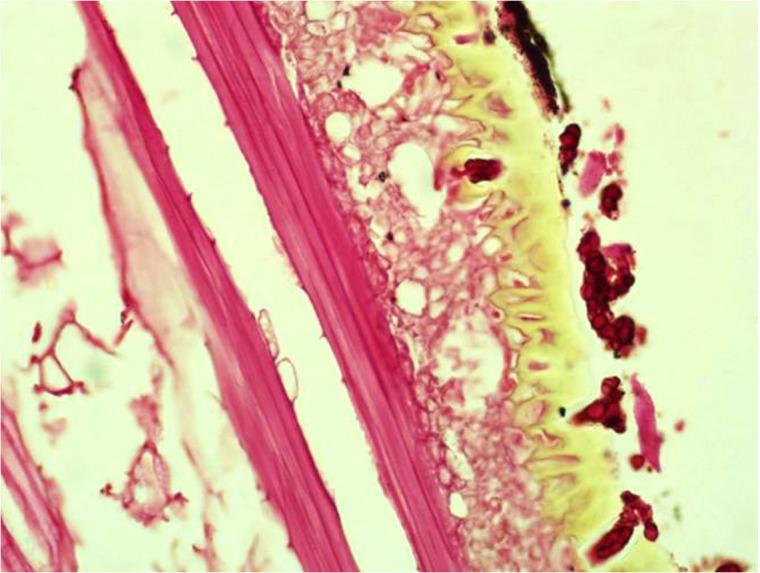
This communication reports on the Mycetoma Research Centre of the University of Khartoum, Sudan experience on 6,792 patients seen during the period 1991-2014.The patients were predominately young (64% under 30 years old) males (76%). The majority (68%) were from the Sudan mycetoma belt and 28% were students. Madurella mycetomatis eumycetoma was the most common type (70%). In 66% of the patients the duration of the disease was less than five years, and 81% gave a history of sinuses discharging mostly black grains (78%). History of trauma at the mycetoma site was reported in 20%. Local pain was reported in 27% of the patients, and only 12% had a family history of mycetoma. The study showed that 57% of the patients had previous surgical excisions and recurrence, and only 4% received previous medical treatment for mycetoma. Other concomitant medical diseases were reported in 4% of the patients. The foot (76%) and hand (8%) were the most commonly affected sites. Less frequently affected sites were the leg and knee (7%), thigh (2%), buttock (2%) and arm and forearm (1%). Rare sites included the chest wall, head and neck, back, abdominal wall, perineum, oral cavity, tongue and eye. Multiple sites mycetoma was recorded in 135 (2%) of cases. At presentation, 37% of patients had massive lesions, 79% had sinuses, 8% had local hyper-hydrosis at the mycetoma lesion, 11% had regional lymphadenopathy, while 6% had dilated tortuous veins proximal to the mycetoma lesions. The diagnosis of mycetoma was established by combined imaging techniques and cytological, histopathological, serological tests and grain culture. Patients with actinomycetoma received a combination of antimicrobial agents, while eumycetoma patients received antifungal agents combined with various surgical excisions. Surgical excisions in the form of wide local excision, debridement or amputation were done in 807 patients, and of them 248 patients (30.7%) had postoperative recurrence. Different types of amputations were done in 120 patients (1.7%).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Fahal AH. (2004) Mycetoma thorn on the flesh. Trans R Soc Trop Med Hyg. 98(1):3–11. - PubMed
-
- Fahal AH, Hassan MA. (1992) Mycetoma. Br J Surg. 79(11): 1138–1141. - PubMed
-
- Bonifaz A, Tirado-Sánchez A, Calderón L, Saúl A, Araiza J, et al. (2014) Mycetoma: experience of 482 cases in a single center in Mexico. PLoS Negl Trop Dis. 21; 8(8):e3102 doi: 10.1371/journal.pntd.0003102. e Collection 2014 - DOI - PMC - PubMed
-
- Ahmed AO, van Leeuwen W, Fahal A, van de Sande W, Verbrugh H, et al. (2004) Mycetoma caused by Madurella mycetomatis: a neglected infectious burden. Lancet Infect Dis. 4(9):566–74. - PubMed
-
- Ahmed AOA, van de Sande WW, Fahal A, Bakker-Woudenberg I, Verbrugh H, et al. (2007) Management of mycetoma: major challenge in tropical mycoses with limited international recognition. Curr Opin Infect Dis. 20(2):146–51. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources