Therapeutic responses of Plasmodium vivax malaria to chloroquine and primaquine treatment in northeastern Myanmar
- PMID: 25512415
- PMCID: PMC4335844
- DOI: 10.1128/AAC.04270-14
Therapeutic responses of Plasmodium vivax malaria to chloroquine and primaquine treatment in northeastern Myanmar
Abstract
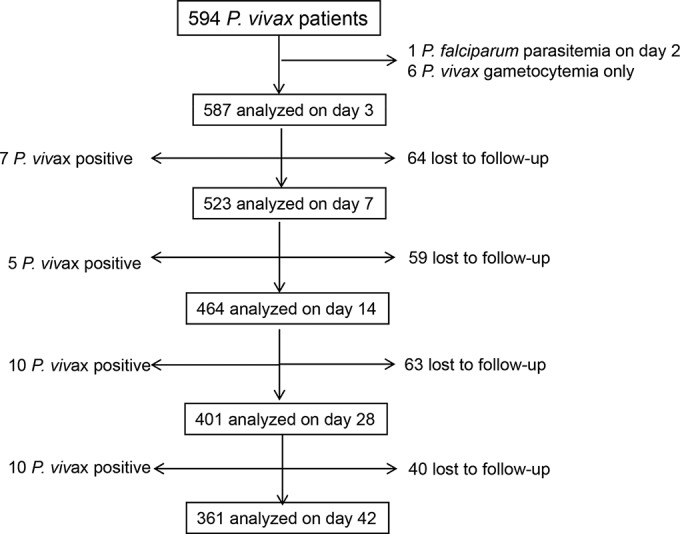
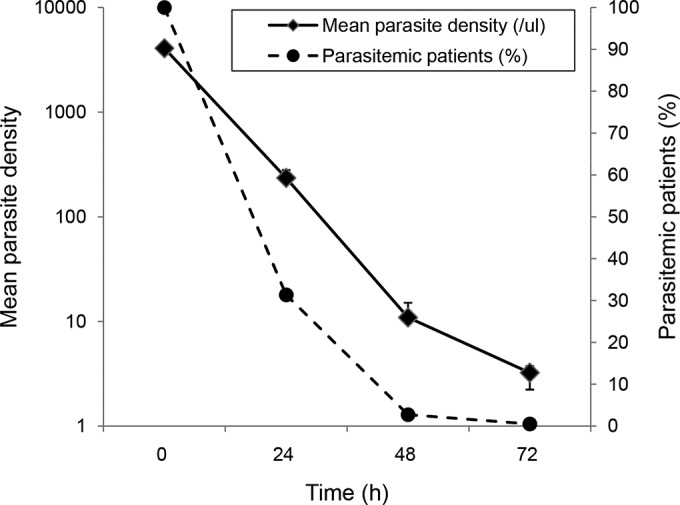
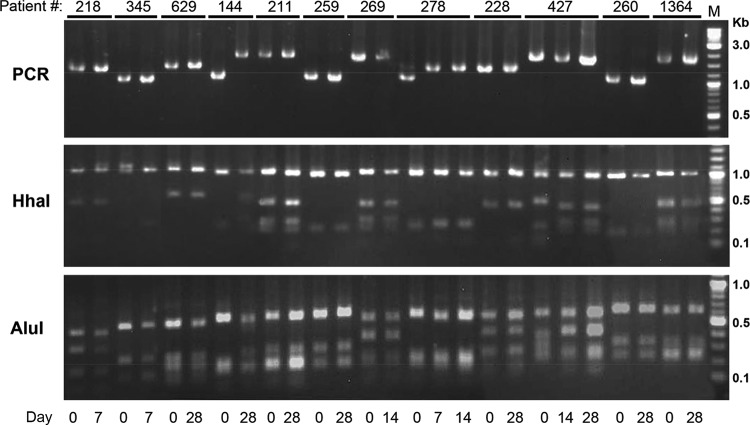
Chloroquine-primaquine (CQ-PQ) continues to be the frontline therapy for radical cure of Plasmodium vivax malaria. Emergence of CQ-resistant (CQR) P. vivax parasites requires a shift to artemisinin combination therapies (ACTs), which imposes a significant financial, logistical, and safety burden. Monitoring the therapeutic efficacy of CQ is thus important. Here, we evaluated the therapeutic efficacy of CQ-PQ for P. vivax malaria in northeast Myanmar. We recruited 587 patients with P. vivax monoinfection attending local malaria clinics during 2012 to 2013. These patients received three daily doses of CQ at a total dose of 24 mg of base/kg of body weight and an 8-day PQ treatment (0.375 mg/kg/day) commencing at the same time as the first CQ dose. Of the 401 patients who finished the 28-day follow-up, the cumulative incidence of recurrent parasitemia was 5.20% (95% confidence interval [CI], 3.04% to 7.36%). Among 361 (61%) patients finishing a 42-day follow-up, the cumulative incidence of recurrent blood-stage infection reached 7.98% (95% CI, 5.20% to 10.76%). The cumulative risk of gametocyte carriage at days 28 and 42 was 2.21% (95% CI, 0.78% to 3.64%) and 3.93% (95% CI, 1.94% to 5.92%), respectively. Interestingly, for all 15 patients with recurrent gametocytemia, this was associated with concurrent asexual stages. Genotyping of recurrent parasites at the merozoite surface protein 3α gene locus from 12 patients with recurrent parasitemia within 28 days revealed that 10 of these were the same genotype as at day 0, suggesting recrudescence or relapse. Similar studies in 70 patients in the same area in 2007 showed no recurrent parasitemias within 28 days. The sensitivity to chloroquine of P. vivax in northeastern Myanmar may be deteriorating.
Copyright © 2015, American Society for Microbiology. All Rights Reserved.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- Gething PW, Elyazar IR, Moyes CL, Smith DL, Battle KE, Guerra CA, Patil AP, Tatem AJ, Howes RE, Myers MF, George DB, Horby P, Wertheim HF, Price RN, Mueller I, Baird JK, Hay SI. 2012. A long neglected world malaria map: Plasmodium vivax endemicity in 2010. PLoS Negl Trop Dis 6:e1814. doi:10.1371/journal.pntd.0001814. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources