A comprehensive assessment of lymphatic filariasis in Sri Lanka six years after cessation of mass drug administration
- PMID: 25393404
- PMCID: PMC4230885
- DOI: 10.1371/journal.pntd.0003281
A comprehensive assessment of lymphatic filariasis in Sri Lanka six years after cessation of mass drug administration
Erratum in
- PLoS Negl Trop Dis. 2014 Dec;(12):e3428
Abstract
Background: The Sri Lankan Anti-Filariasis Campaign conducted 5 rounds of mass drug administration (MDA) with diethycarbamazine plus albendazole between 2002 and 2006. We now report results of a comprehensive surveillance program that assessed the lymphatic filariasis (LF) situation in Sri Lanka 6 years after cessation of MDA.
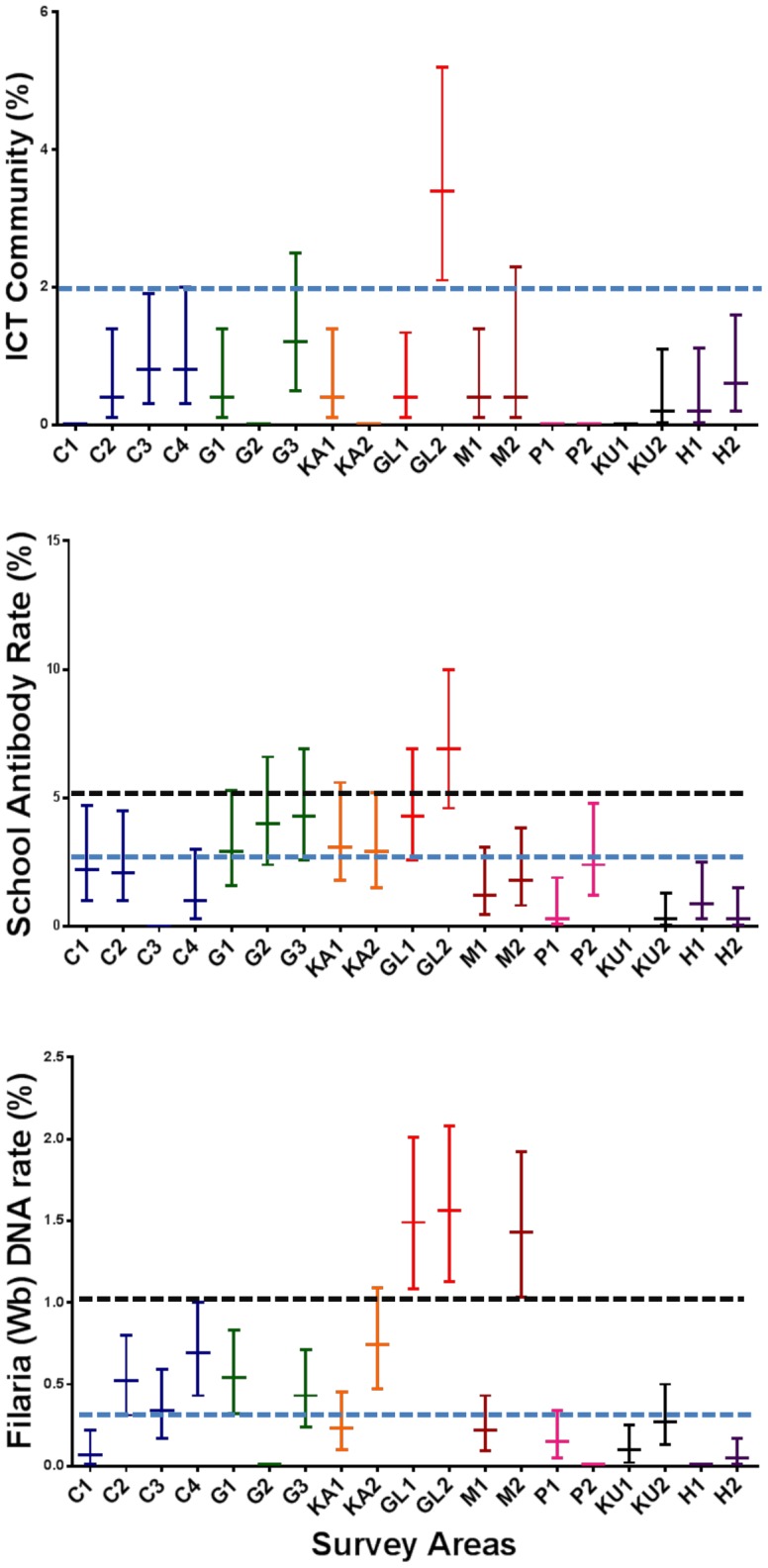
Methodology and principal findings: Transmission assessment surveys (TAS) were performed per WHO guidelines in primary school children in 11 evaluation units (EUs) in all 8 formerly endemic districts. All EUs easily satisfied WHO criteria for stopping MDA. Comprehensive surveillance was performed in 19 Public Health Inspector (PHI) areas (subdistrict health administrative units). The surveillance package included cross-sectional community surveys for microfilaremia (Mf) and circulating filarial antigenemia (CFA), school surveys for CFA and anti-filarial antibodies, and collection of Culex mosquitoes with gravid traps for detection of filarial DNA (molecular xenomonitoring, MX). Provisional target rates for interruption of LF transmission were community CFA <2%, antibody in school children <2%, and filarial DNA in mosquitoes <0.25%. Community Mf and CFA prevalence rates ranged from 0-0.9% and 0-3.4%, respectively. Infection rates were significantly higher in males and lower in people who denied prior treatment. Antibody rates in school children exceeded 2% in 10 study sites; the area that had the highest community and school CFA rates also had the highest school antibody rate (6.9%). Filarial DNA rates in mosquitoes exceeded 0.25% in 10 PHI areas.
Conclusions: Comprehensive surveillance is feasible for some national filariasis elimination programs. Low-level persistence of LF was present in all study sites; several sites failed to meet provisional endpoint criteria for LF elimination, and follow-up testing will be needed in these areas. TAS was not sensitive for detecting low-level persistence of filariasis in Sri Lanka. We recommend use of antibody and MX testing as tools to complement TAS for post-MDA surveillance.
Conflict of interest statement
The filarial antigen test used in this study uses reagents licensed from Barnes-Jewish Hospital, an affiliation of GJW. All royalties from sales of these tests go to the Barnes Jewish Hospital Foundation, a not for profit charitable organization (
Figures
{kind=link}
{kind=link}
References
-
- WHO (2013) Global programme to eliminate lymphatic filariasis: progress report for 2012. Wkly Epidemiol Rec 88: 389–399. - PubMed
-
- Abdulcader MH, Sasa M (1966) Epidemiology and control of bancroftian filariasis in Ceylon. Jpn J Exp Med 36: 609–646. - PubMed
-
- Schweinfurth U (1983) Filarial diseases in Ceylon: a geographic and historical analysis. Ecol Dis 2: 309–319. - PubMed
-
- Dissanaike AS (1991) Filariasis in Ceylon then (1961) and in Sri Lanka now (1990–30 years on). Ann Trop Med Parasitol 85: 123–129. - PubMed
-
- AntifilariasisCampaign (2013) Annual reports. Ministry of Health, Sri Lanka Available at http://wwwfilariasiscampaignhealthgovlk/subpgs/03_reportshtml.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical