APOL1 kidney risk alleles: population genetics and disease associations
- PMID: 25168832
- PMCID: PMC4157456
- DOI: 10.1053/j.ackd.201406005
APOL1 kidney risk alleles: population genetics and disease associations
Abstract
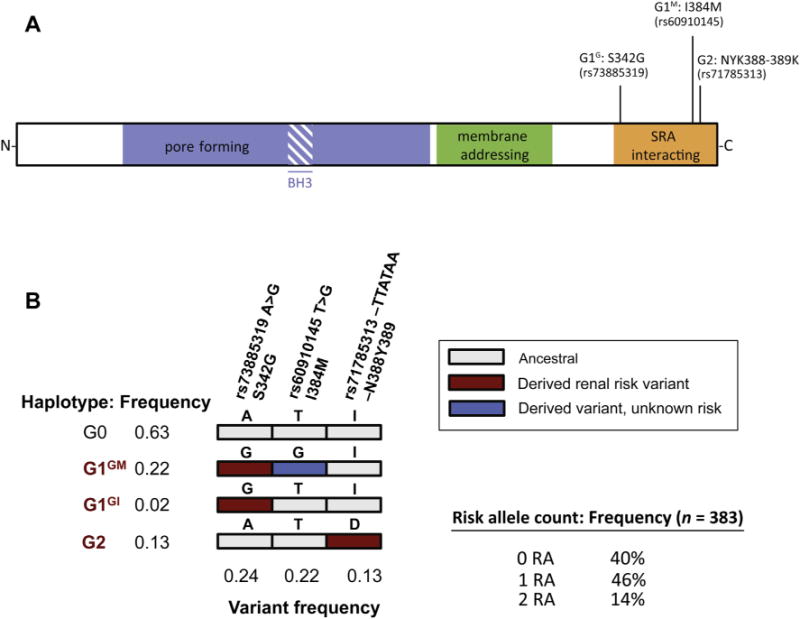
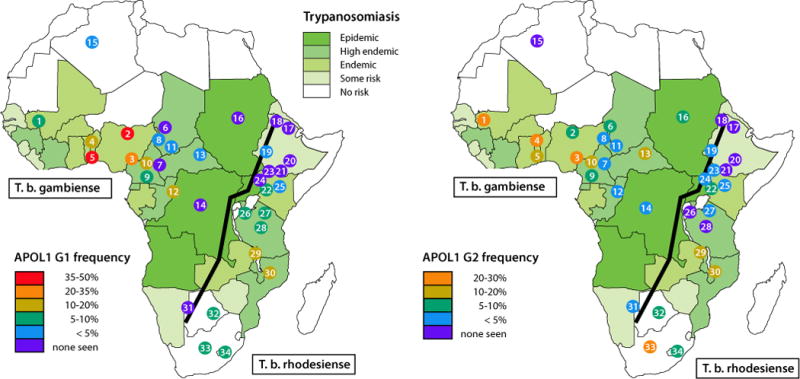
APOL1 kidney disease is a unique case in the field of the genetics of common disease: 2 variants (termed G1 and G2) with high population frequency have been repeatedly associated with nondiabetic CKDs, with very strong effect size (odds ratios 3-29) in populations of sub-Saharan African descent. This review provides an update on the spectrum of APOL1 kidney disease and on the worldwide distribution of these kidney risk variants. We also summarize the proper way to run a recessive analysis on joint and independent effects of APOL1 G1 and G2 kidney risk variants.
Keywords: APOL1 demographics; African admixture; Apolipoprotein L1; Chronic kidney disease; Glomerular disease.
Copyright © 2014 National Kidney Foundation, Inc. All rights reserved.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- Vanhamme L, Paturiaux-Hanocq F, Poelvoorde P, et al. Apolipoprotein L-I is the trypanosome lytic factor of human serum. Nature. 2003;422(6927):83–87. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous