The lost hope of elimination of Kala-azar (visceral leishmaniasis) by 2010 and cyclic occurrence of its outbreak in India, blame falls on vector control practices or co-infection with human immunodeficiency virus or therapeutic modalities?
- PMID: 24754021
- PMCID: PMC3992795
- DOI: 10.4103/2229-5070.129143
The lost hope of elimination of Kala-azar (visceral leishmaniasis) by 2010 and cyclic occurrence of its outbreak in India, blame falls on vector control practices or co-infection with human immunodeficiency virus or therapeutic modalities?
Abstract
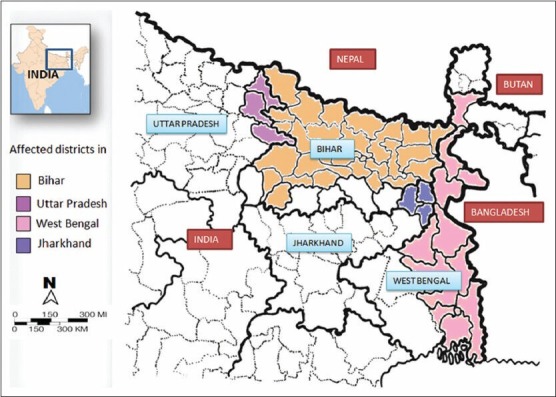
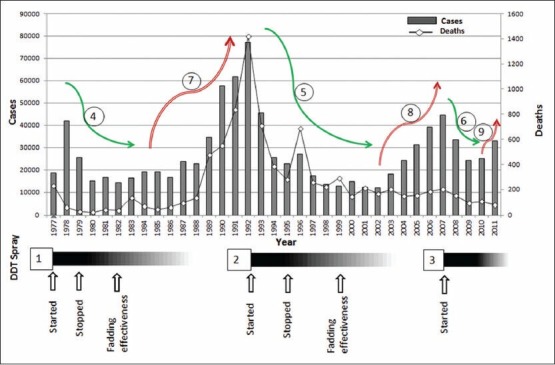
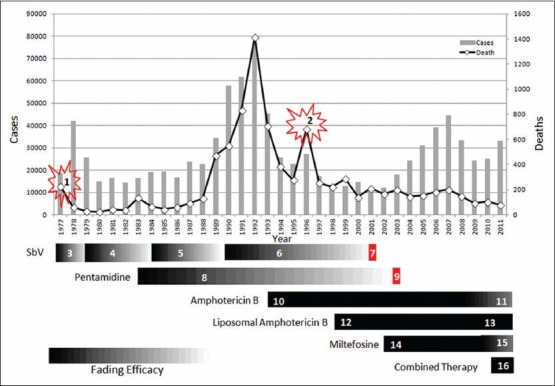
The Kala-azar/visceral leishmaniasis (VL) turns epidemic form once in every 15 years in the endemic regions of Indian subcontinent. The goal of elimination of Kala-azar from India by 2010 was lost despite paramount efforts taken by the Government of India and World Health Organization and Regional Office for South East Asia. The main objective of this review was to elucidate the possible reason for the failure of Kala-azar elimination program and to suggest possible remedial measures to achieve the goal in future. The annual numbers of VL cases and deaths recorded in India since 1977 were plotted on a graph, to see if the temporal trends could be associated with changes in the vector control practices or co-infection with human immunodeficiency virus (HIV) or therapeutic modalities used against VL. The VL cases flares up whenever the effect of dichlorodiphenyltrichloroethane (DDT) diminished after the withdrawal of spray. The fading effectiveness was clearly correlated with an increasing number of VL cases. Therapeutic modalities were found to be highly correlating with VL mortality not with VL morbidity. The diminishing efficacy of first and second line drugs and the introduction of new drugs and drugs combination were responsible for ups and downs in the VL mortality. The VL mortality is constantly declining since 1993, but cases started increasing from 2003 to 2007 and then recently again from 2010 to 2011. This shows a serious lacuna in the vector control practices applied. The extent of HIV co-infection did not show any correlation with number/trend of VL cases or death over the study period. It is concluded that, by strict vector control practices, the VL cases can be reduced and by applying proper therapeutic strategies, the VL mortality can be reduced. HIV-VL co-infection does not seem to be in a worried stage.
Keywords: Co-infection; Kala-azar; cyclic occurrence; elimination; human immunodeficiency virus; therapeutic modalities; vector control practices; visceral leishmaniasis.
Conflict of interest statement
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- WHO. Leishmaniasis home. 2011. [Last accessed on 2011 Jun 6]. Available from: http://www.who.int/leishmaniasis/en/
-
- Cox FE, Kreier JP, Wakelin D. Parasitology. In: Collier L, Balows A, Sussman M, editors. Topley and Wilson's Microbiology and Microbial Infections. Vol. 5. 338, Euston Road, London NWI 3BH: Hodder Arnold; 1998.
-
- Bhattacharya SK, Sur D, Sinha PK, Karbwang J. Elimination of leishmaniasis (kala-azar) from the Indian subcontinent is technically feasible and operationally achievable. Indian J Med Res. 2006;123:195–6. - PubMed
-
- Alvar J, Yactayo S, Bern C. Leishmaniasis and poverty. Trends Parasitol. 2006;22:552–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous