Measuring underreporting and under-ascertainment in infectious disease datasets: a comparison of methods
- PMID: 24517715
- PMCID: PMC4015559
- DOI: 10.1186/1471-2458-14-147
Measuring underreporting and under-ascertainment in infectious disease datasets: a comparison of methods
Abstract
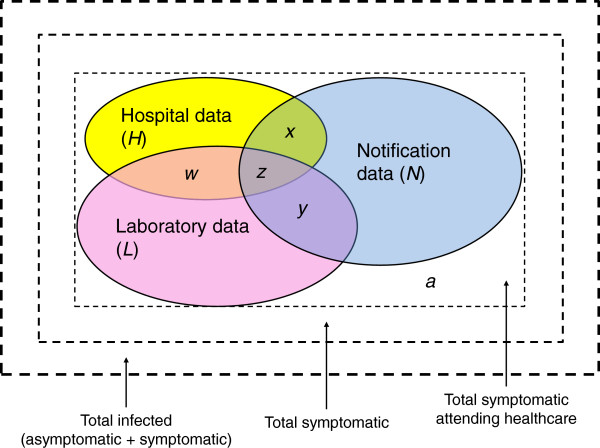
Background: Efficient and reliable surveillance and notification systems are vital for monitoring public health and disease outbreaks. However, most surveillance and notification systems are affected by a degree of underestimation (UE) and therefore uncertainty surrounds the 'true' incidence of disease affecting morbidity and mortality rates. Surveillance systems fail to capture cases at two distinct levels of the surveillance pyramid: from the community since not all cases seek healthcare (under-ascertainment), and at the healthcare-level, representing a failure to adequately report symptomatic cases that have sought medical advice (underreporting). There are several methods to estimate the extent of under-ascertainment and underreporting.
Methods: Within the context of the ECDC-funded Burden of Communicable Diseases in Europe (BCoDE)-project, an extensive literature review was conducted to identify studies that estimate ascertainment or reporting rates for salmonellosis and campylobacteriosis in European Union Member States (MS) plus European Free Trade Area (EFTA) countries Iceland, Norway and Switzerland and four other OECD countries (USA, Canada, Australia and Japan). Multiplication factors (MFs), a measure of the magnitude of underestimation, were taken directly from the literature or derived (where the proportion of underestimated, under-ascertained, or underreported cases was known) and compared for the two pathogens.
Results: MFs varied between and within diseases and countries, representing a need to carefully select the most appropriate MFs and methods for calculating them. The most appropriate MFs are often disease-, country-, age-, and sex-specific.
Conclusions: When routine data are used to make decisions on resource allocation or to estimate epidemiological parameters in populations, it becomes important to understand when, where and to what extent these data represent the true picture of disease, and in some instances (such as priority setting) it is necessary to adjust for underestimation. MFs can be used to adjust notification and surveillance data to provide more realistic estimates of incidence.
Figures
{kind=link}
{kind=link}
References
-
- Wheeler JG, Sethi D, Cowden JM, Wall PG, Rodrigues LC, Tompkins DS, Hudson MJ, Roderick PJ. Study of infectious intestinal disease in England: rates in the community, presenting to general practice, and reported to national surveillance. BMJ. 1999;318(7190):1046–1050. doi: 10.1136/bmj.318.7190.1046. - DOI - PMC - PubMed
-
- Mangen M-JJ, Plass D, Havelaar AH, Gibbons CL, Cassini A, Mühlberger N, van Lier A, Haagsma JA, Brooke RJ, Lai T. et al.The Pathogen- and Incidence-Based DALY Approach: An Appropriated Methodology for Estimating the Burden of Infectious Diseases. PLoS ONE. 2013;8(11):e79740. doi: 10.1371/journal.pone.0079740. - DOI - PMC - PubMed
-
- Plass D, Mangen M-JJ, Havelaar AH, Gibbons C, Haagsma J, Jahn B, Lai T, van Lier A, Longhi S, McDonald SA. et al.The incidence-based and pathogen-based disability-adjusted life-years approach for measuring infectious disease burden in Europe: the burden of communicable diseases in Europe (BCoDE) project. Lancet. 2013;381:S114.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical