Cytokine network in scrub typhus: high levels of interleukin-8 are associated with disease severity and mortality
- PMID: 24516677
- PMCID: PMC3916254
- DOI: 10.1371/journal.pntd.0002648
Cytokine network in scrub typhus: high levels of interleukin-8 are associated with disease severity and mortality
Abstract
Background: Scrub typhus, caused by Orientia tsutsugamushi, is endemic in the Asia-Pacific region. Mortality is high if untreated, and even with treatment as high as 10-20%, further knowledge of the immune response during scrub typhus is needed. The current study was aimed at comparing plasma levels of a variety of inflammatory mediators in scrub typhus patients and controls in South India in order to map the broader cytokine profile and their relation to disease severity and clinical outcome.
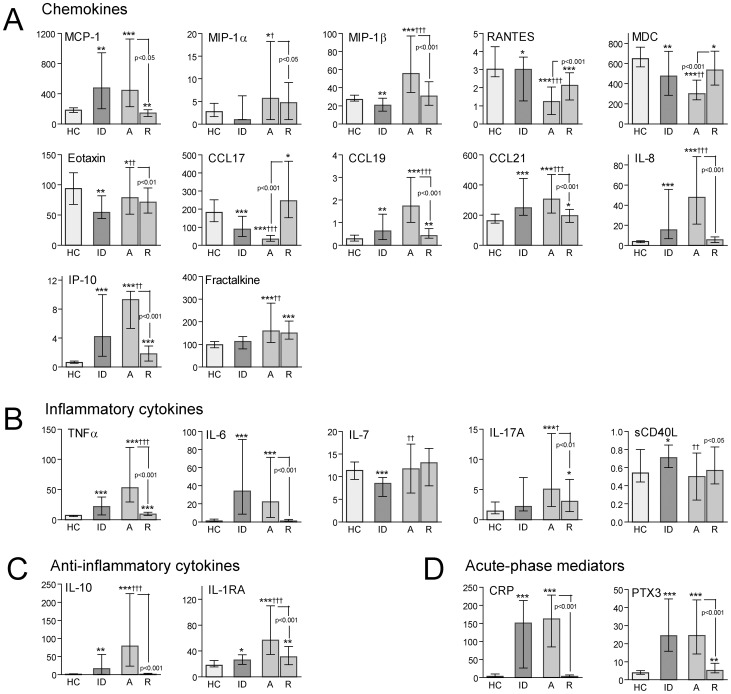
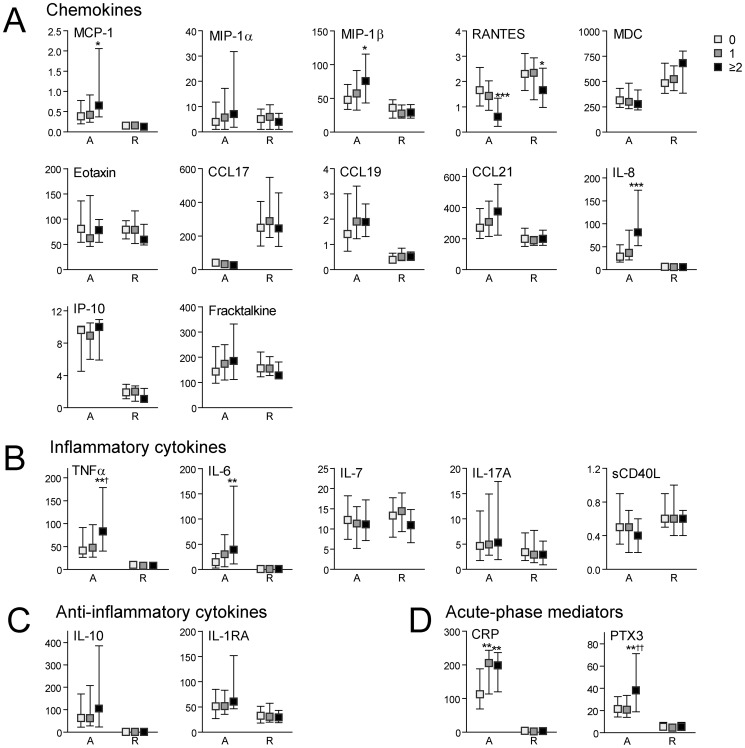
Methodology/principal findings: We examined plasma levels of several cytokines in scrub typhus patients (n = 129) compared to healthy controls (n = 31) and infectious disease controls (n = 31), both in the acute phase and after recovery, by multiplex technology and enzyme immunoassays. Scrub typhus patients were characterized by marked changes in the cytokine network during the acute phase, differing not only from healthy controls but also from infectious disease controls. While most of the inflammatory markers were raised in scrub typhus, platelet-derived mediators such as RANTES were markedly decreased, probably reflecting enhanced platelet activation. Some of the inflammatory markers, including various chemokines (e.g., interleukin-8, monocyte chemoattractant peptide-1 and macrophage inflammatory protein-1β) and downstream markers of inflammation (e.g., C-reactive protein and pentraxin-3), were also associated with disease severity and mortality during follow-up, with a particular strong association with interleukin-8.
Conclusions/significance: Our findings suggest that scrub typhus is characterized by a certain cytokine profile that includes dysregulated levels of a wide range of mediators, and that this enhanced inflammation could contribute to disease severity and clinical outcome.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- Watt G, Parola P (2003) Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis 16 (5) 429–436. - PubMed
-
- Kawamura A Jr, Tanaka H (1988) Rickettsiosis in Japan. Jpn J Exp Med 58: 169–184. - PubMed
-
- Varghese GM, Abraham OC, Mathai D, Thomas K, Aaron R, et al. (2006) Scrub typhus among hospitalised patients with febrile illness in South India: magnitude and clinical predictors. J Infect 52: 56–60. - PubMed
-
- Kumar K, Saxena VK, Thomas TG, Lal S (2004) Outbreak investigation of scrub Typhus in Himachal Pradesh (India). J Commun Dis 36: 277–283. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials