Post kala-azar dermal leishmaniasis: an unresolved mystery
- PMID: 24388776
- PMCID: PMC3919212
- DOI: 10.1016/j.pt.201312004
Post kala-azar dermal leishmaniasis: an unresolved mystery
Abstract
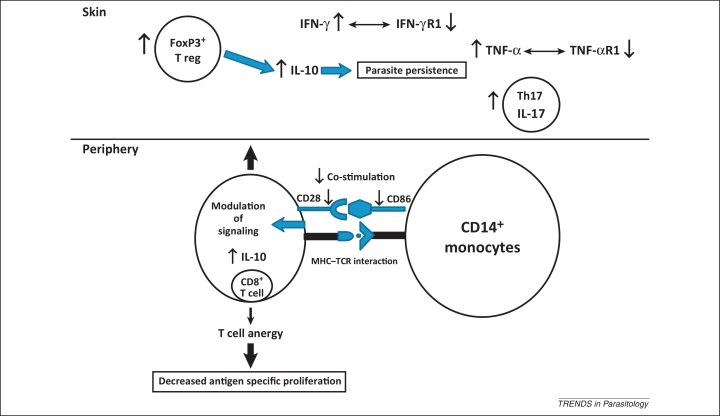
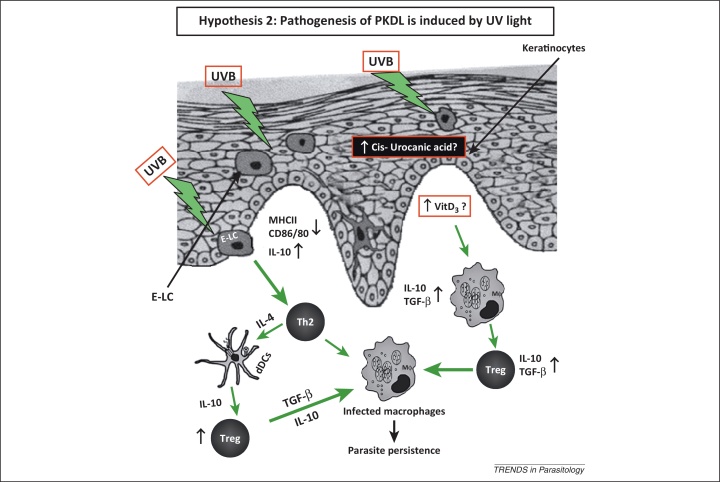
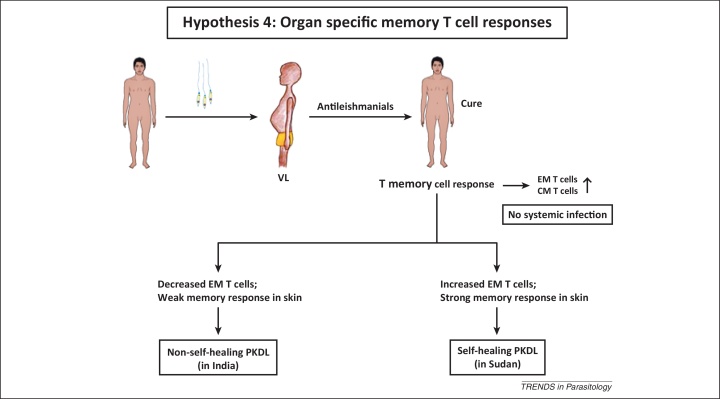
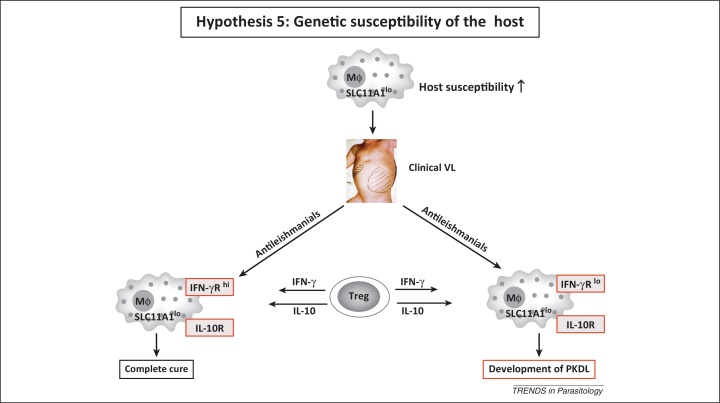
Post kala-azar dermal leishmaniasis (PKDL), a cutaneous sequela of visceral leishmaniasis (VL), develops in some patients alongside but more commonly after apparent cure from VL. In view of the pivotal role of PKDL patients in the transmission of VL, here we review clinical, epidemiological, parasitological, and immunological perspectives of this disease, focusing on five hypotheses to explain the development of PKDL: (i) the role of antimonial drugs; (ii) UV-induced skin damage; (iii) reinfection; (iv) organ specific failure of memory T cell responses; and (v) genetic susceptibility of the host. This review will enable researchers and clinicians to explore the unresolved mystery of PKDL and provide a framework for future application of 'omic' approaches for the control and eventual elimination of VL.
Keywords: UV light; antimony; post kala-azar dermal leishmaniasis (PKDL); regulatory T cells; vitamin D.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Antinori S. Post kala-azar dermal leishmaniasis as an immune reconstitution inflammatory syndrome in a patient with acquired immune deficiency syndrome. Br. J. Dermatol. 2007;157:1032–1036. - PubMed
-
- Ganguly S. Post kala-azar dermal leishmaniasis – an overview. Int. J. Dermatol. 2010;49:921–931. - PubMed
-
- Desjeux P., Ramesh V. In: Kala Azar in South Asia – Current Status and Challenges Ahead. Jha T.K., Noiri E., editors. Springer; 2011. Post kala-azar dermal leishmaniasis: facing the challenge of eliminating kala-azar from South Asia; pp. 111–124.
-
- Zijlstra E.E. Post kala-azar dermal leishmaniasis. Lancet Infect. Dis. 2003;3:87–98. - PubMed
-
- Mondal D., Khan M.G. Recent advances in post kala-azar dermal leishmaniasis. Curr. Opin. Infect. Dis. 2011;24:418–422. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources