Clinical and laboratory characteristics of severe fever with thrombocytopenia syndrome in Chinese patients
- PMID: 24076112
- PMCID: PMC9425216
- DOI: 10.1016/j.bjid.2013年05月01日1
Clinical and laboratory characteristics of severe fever with thrombocytopenia syndrome in Chinese patients
Abstract
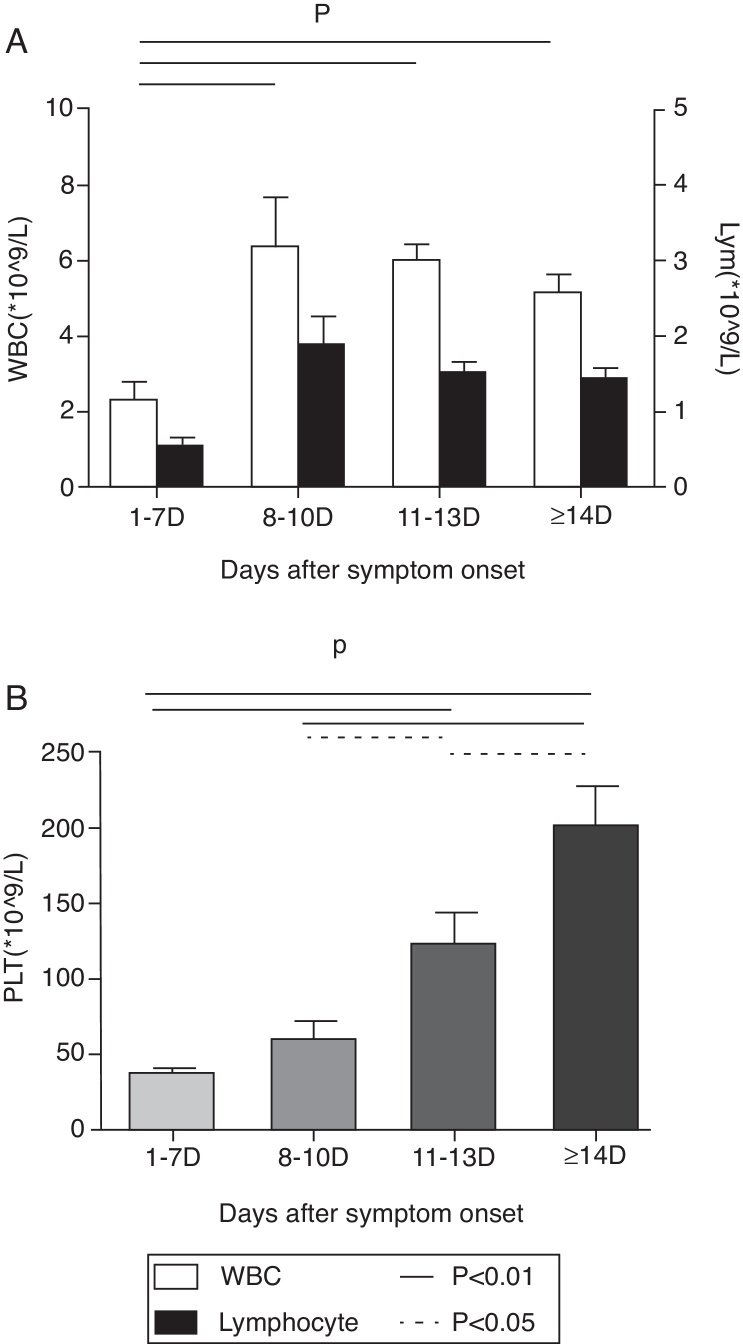
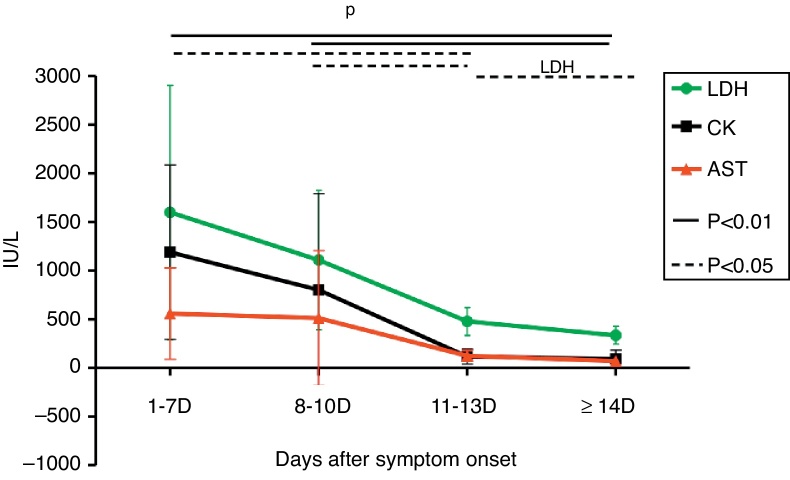
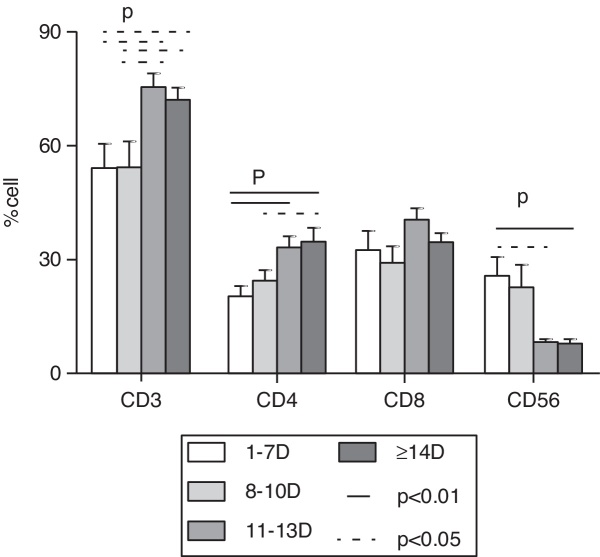
Severe fever with thrombocytopenia syndrome (SFTS) associated with severe fever with thrombocytopenia syndrome virus (SFTSV) is an emerging infectious disease. 12 patients with severe fever with thrombocytopenia syndrome in our study were presented mainly with fever and severe malaise. The clinical manifestations typically became worse on the 6th or 7th day. The average fever time is 9.11 ± 1.54 days. Most of them had multiorgan dysfunction, and part of them had hemophagocytic lymphohistiocytosis histiocytosis (HLH). The characteristic laboratory findings in the early stage were the drop of white blood cells (WBC), platelets (PLT) and serum Ca++, while increase of aspartate amino transferase (AST), creatine kinase (CK), and lactate dehydrogenase (LDH). CD3+CD4+ were significantly decreased, while CD3-CD56+ were significantly increased, whereas CD3+CD8+ were constantly elevated throughout the disease course. Ten to 14 days after illness onset, symptoms were improved, accompanied by resolution of laboratory abnormalities. These results indicate that severe fever with thrombocytopenia syndrome has an acute onset and self-limited course. It is a systemic infection. The host immune response caused tissues and organs injury. The improvement of symptoms and laboratory tests is consistent with the elimination of the virus and recover of immune response. Further investigation should be done in order to better understand this disease and guide the clinical treatment.
Keywords: Bunyaviridae infection; Clinical features; Laboratory characteristics; Thrombocytopenia.
Copyright © 2013 Elsevier Editora Ltda. All rights reserved.
Figures
{kind=link}
{kind=link}
{kind=link}
References
-
- Bao C.-j., Guo X.-l., Qi X., et al. A family cluster of infections by a newly recognized bunyavirus in Eastern China, 2007: further evidence of person-to-person transmission. Clin Infect Dis. 2011;53:1208–1214. - PubMed
-
- Chen N., Weng Y., Li J. Hemophagocytic lymphohistiocytosis associated with novel bunyavirus infection – case report. Chin J Clin Infect Dis. 2011;4:269–270.
-
- Zhang Y.-Z., Zhou D.-J., Xiong Y.-w., et al. Hemorrhagic fever caused by a novel tick-borne Bunyavirus in Huaiyangshan. China. Chin J Epidemiol. 2011;32:209–220. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials