Immunopathologic characterization of naturally acquired Trypanosoma cruzi infection and cardiac sequalae in cynomolgus macaques (Macaca fascicularis)
- PMID: 24041209
- PMCID: PMC3784659
Immunopathologic characterization of naturally acquired Trypanosoma cruzi infection and cardiac sequalae in cynomolgus macaques (Macaca fascicularis)
Abstract
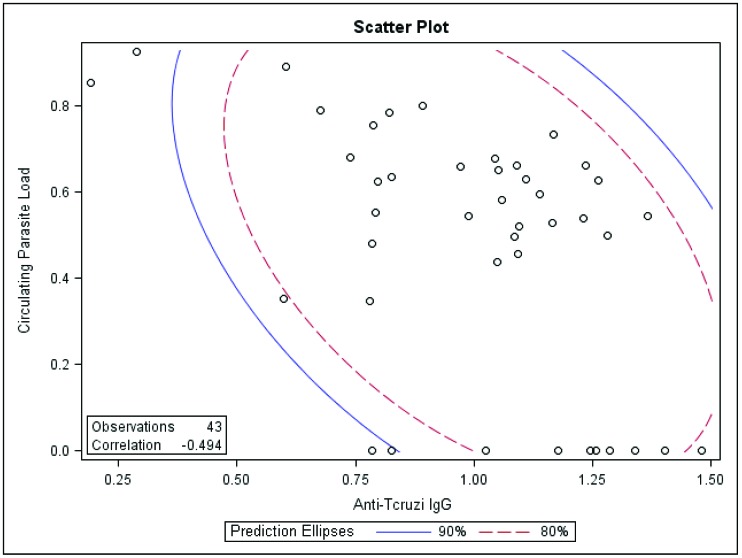
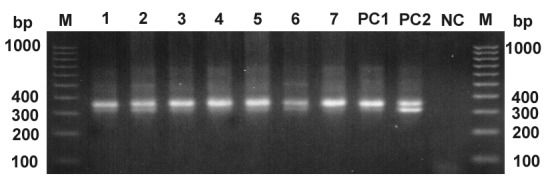
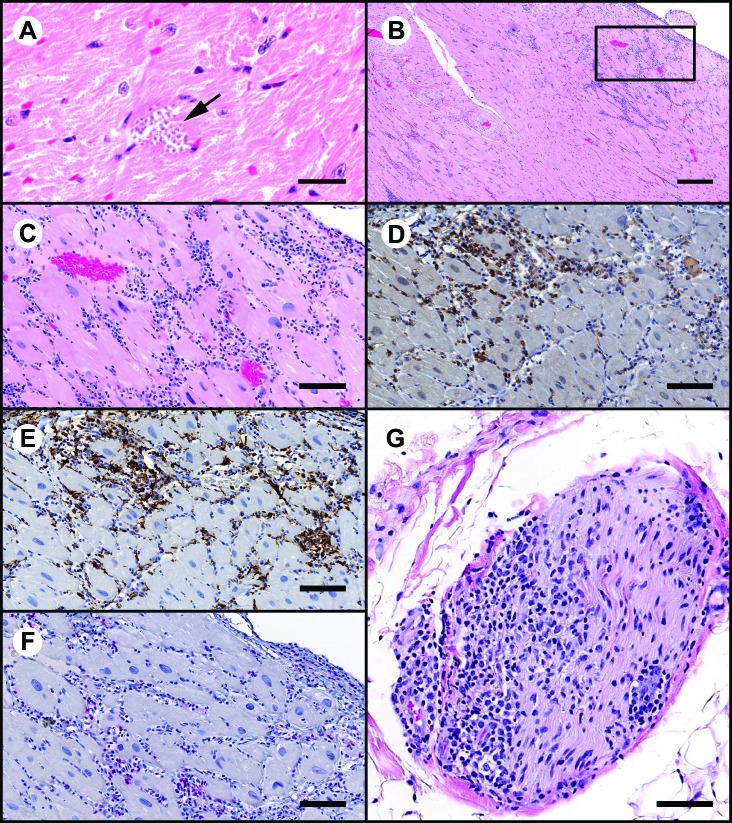
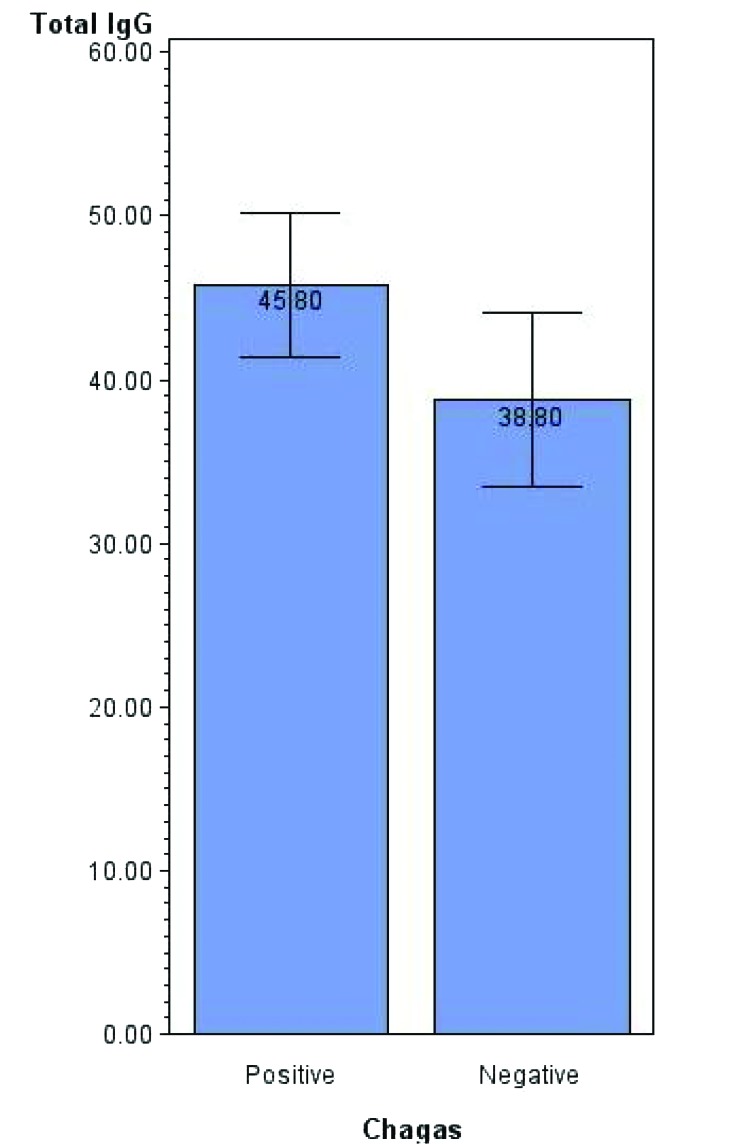
Trypanosoma cruzi, the causative agent of Chagas disease, is endemic in south Texas due to the abundant vector and wild small mammalian reservoir populations. This situation predisposes nonhuman primate colonies exposed to outdoor housing to infection from ingestion or bite of triatomid insects. Using a T. cruzi-specific real-time PCR and Trypanosome spp.-specific ELISA, we revealed a prevalence rate of 8.5% in a colony of outdoor-housed cynomolgus macaques. By using a discriminating kinetoplastid minicircle PCR, we eliminated the possibility of mixed prevalence with nonpathogenic trypanosomes and showed the ELISA results were specific for T. cruzi. In this study, we found an inverse relationship between antibody titers and circulating parasite load. Also, 23% of T. cruzi IgG ELISA-positive macaques were negative by real-time PCR. Furthermore, in a subset of infected macaques, cardiac tissue was infiltrated by inflammatory mononuclear cells and contained T. cruzi genomic and kinetoplast DNA despite lacking microscopic evidence of discrete parasite stages. In addition, 19% of the infected macaques had titers for cardiac troponin I autoantibody, which could contribute to autoimmune myocarditis or interfere with circulating troponin I measurements. These findings indicate the possibility of T. cruzi to interfere with the assessment of cardiac safety signals in preclinical toxicology and safety pharmacology studies and the necessity for prestudy screening for T. cruzi in outdoor-housed nonhuman primates from endemic areas.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Avila JL. 1992. Molecular mimicry between Trypanosoma cruzi and host nervous tissues. Acta Cient Venez 43:330–340 - PubMed
-
- Bermejo DA, Amezcua Vesely MC, Khan M, Acosta Rodriguez EV, Montes CL, Merino MC, Toellner KM, Mohr E, Taylor D, Cunningham AF, Gruppi A. 2011. Trypanosoma cruzi infection induces a massive extrafollicular and follicular splenic B-cell response which is a high source of nonparasite-specific antibodies. Immunology 132:123–133 - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous