Mass treatment with azithromycin for trachoma: when is one round enough? Results from the PRET Trial in the Gambia
- PMID: 23785525
- PMCID: PMC3681669
- DOI: 10.1371/journal.pntd.0002115
Mass treatment with azithromycin for trachoma: when is one round enough? Results from the PRET Trial in the Gambia
Erratum in
- PLoS Negl Trop Dis. 2013 Jun;7(6). doi:10.1371/annotation/0bae8b34-5ae7-4044-a071-8d88d520a01b
Abstract
Background: The World Health Organization has recommended three rounds of mass drug administration (MDA) with antibiotics in districts where the prevalence of follicular trachoma (TF) is ≥10% in children aged 1-9 years, with treatment coverage of at least 80%. For districts at 5-10% TF prevalence it was recommended that TF be assessed in 1-9 year olds in each community within the district, with three rounds of MDA provided to any community where TF≥10%. Worldwide, over 40 million people live in districts whose TF prevalence is estimated to be between 5 and 10%. The best way to treat these districts, and the optimum role of testing for infection in deciding whether to initiate or discontinue MDA, are unknown.
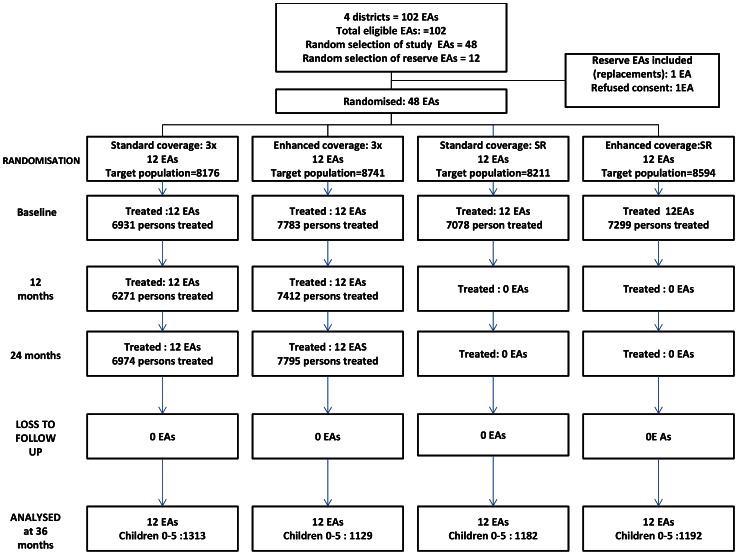
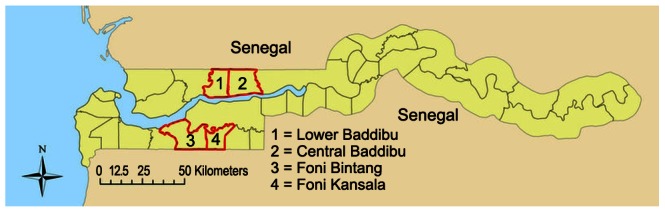
Methods: In a community randomized trial with a factorial design, we randomly assigned 48 communities in four Gambian districts, in which the prevalence of trachoma was known or suspected to be above 10%, to receive annual mass treatment with expected coverage of 80-89% ("Standard"), or to receive an additional visit in an attempt to achieve coverage of 90% or more ("Enhanced"). The same 48 communities were randomised to receive mass treatment annually for three years ("×ばつ"), or to have treatment discontinued if Chlamydia trachomatis (Ct) infection was not detected in a sample of children in the community after mass treatment (stopping rule("SR")). Primary outcomes were the prevalence of TF and of Ct infection in 0-5 year olds at 36 months.
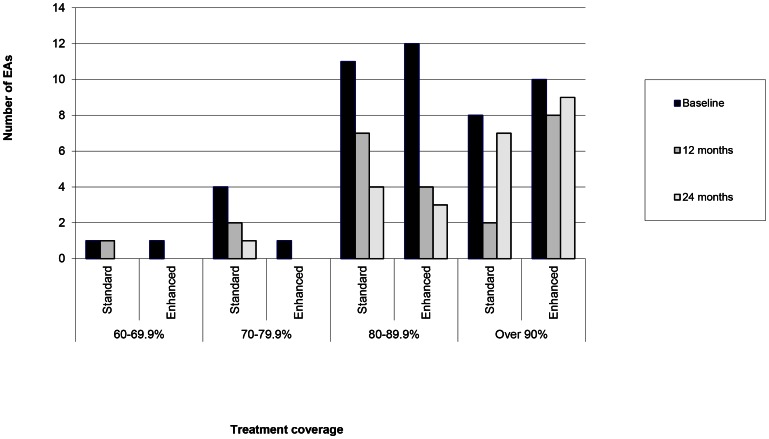
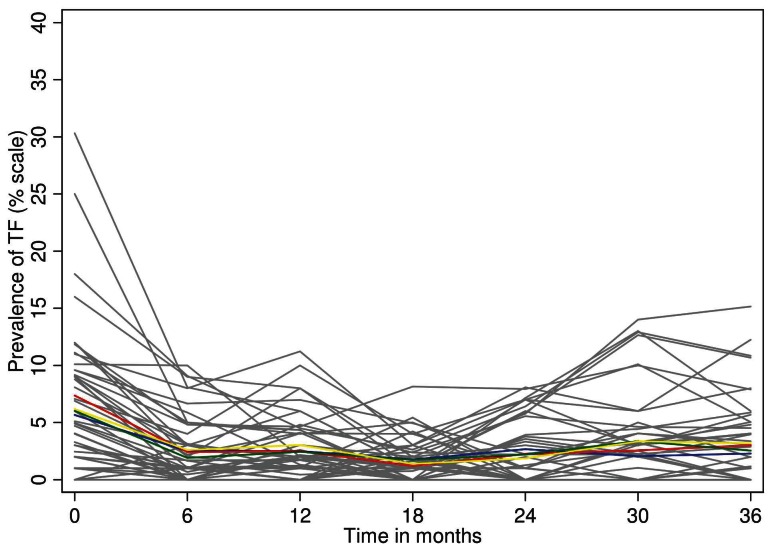
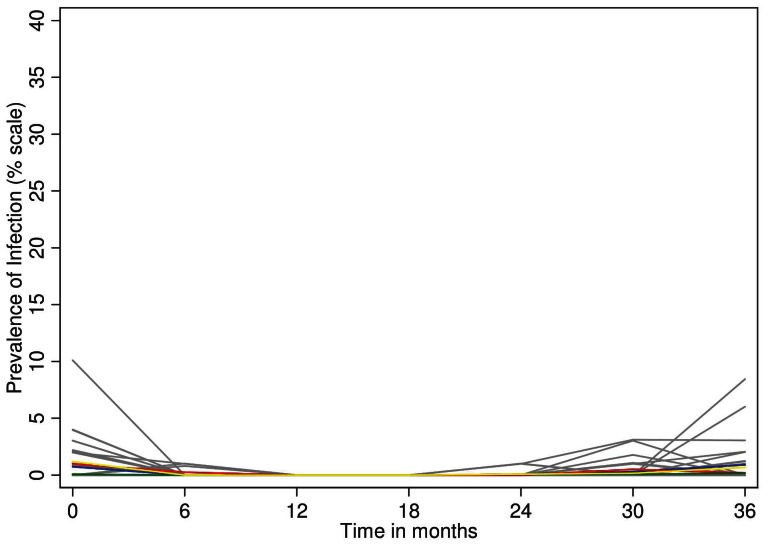
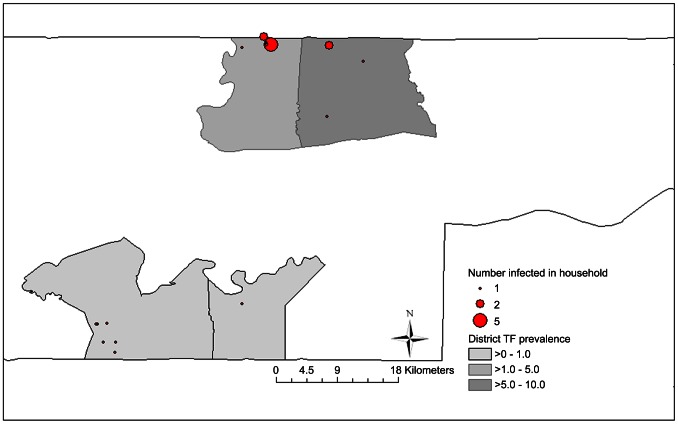
Results: The baseline prevalence of TF and of Ct infection in the target communities was 6.5% and 0.8% respectively. At 36 months the prevalence of TF was 2.8%, and that of Ct infection was 0.5%. No differences were found between the arms in TF or Ct infection prevalence either at baseline (Standard×ばつ: TF 5.6%, Ct 0.7%; Standard-SR: TF 6.1%, Ct 0.2%; Enhanced×ばつ: TF 7.4%, Ct 0.9%; and Enhanced-SR: TF 6.2%, Ct 1.2%); or at 36 months (Standard×ばつ: TF 2.3%, Ct 1.0%; Standard-SR TF 2.5%, Ct 0.2%; Enhanced×ばつ TF 3.0%, Ct 0.2%; and Enhanced-SR TF 3.2%, Ct 0.7% ). The implementation of the stopping rule led to treatment stopping after one round of MDA in all communities in both SR arms. Mean treatment coverage of children aged 0-9 in communities randomised to standard treatment was 87.7% at baseline and 84.8% and 88.8% at one and two years, respectively. Mean coverage of children in communities randomized to enhanced treatment was 90.0% at baseline and 94.2% and 93.8% at one and two years, respectively. There was no evidence of any difference in TF or Ct prevalence at 36 months resulting from enhanced coverage or from one round of MDA compared to three.
Conclusions: The Gambia is close to the elimination target for active trachoma. In districts prioritised for three MDA rounds, one round of MDA reduced active trachoma to low levels and Ct infection was not detectable in any community. There was no additional benefit to giving two further rounds of MDA. Programmes could save scarce resources by determining when to initiate or to discontinue MDA based on testing for Ct infection, and one round of MDA may be all that is necessary in some settings to reduce TF below the elimination threshold.
Trial registration: ClinicalTrials.gov NCT00792922.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Pascolini D, Mariotti SP (2011) Global estimates of visual impairment: 2010. Br J Ophthalmol 65: 614–8. - PubMed
-
- WHO (2012) Global WHO Alliance for the Elimination of Blinding Trachoma by 2020 Progress report on eliminationof trachoma, 2010. Weekly Epidemiological Record 87: 161–168. - PubMed
-
- WHO (1998) World Health Assembly Resolution 51.11. Geneva: WHO.
-
- WHO (2006) Trachoma control - a guide for programme managers. Geneva, Switzerland: World Health Organization.
-
- ITI (2012) ITI- Fighting Blinding Trachoma http://trachoma.org/iti-fighting-blinding-trachoma.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous