Analytical performance of a multiplex Real-Time PCR assay using TaqMan probes for quantification of Trypanosoma cruzi satellite DNA in blood samples
- PMID: 23350002
- PMCID: PMC3547845
- DOI: 10.1371/journal.pntd.0002000
Analytical performance of a multiplex Real-Time PCR assay using TaqMan probes for quantification of Trypanosoma cruzi satellite DNA in blood samples
Abstract
Background: The analytical validation of sensitive, accurate and standardized Real-Time PCR methods for Trypanosoma cruzi quantification is crucial to provide a reliable laboratory tool for diagnosis of recent infections as well as for monitoring treatment efficacy.
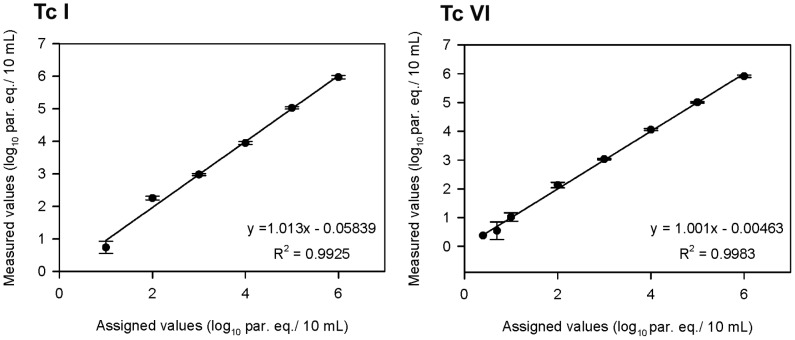
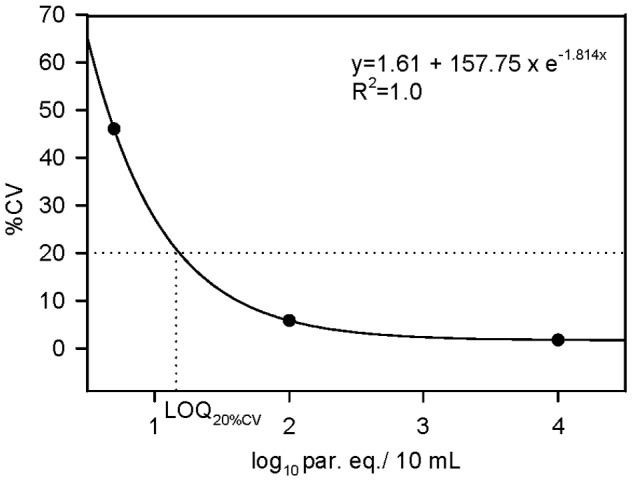
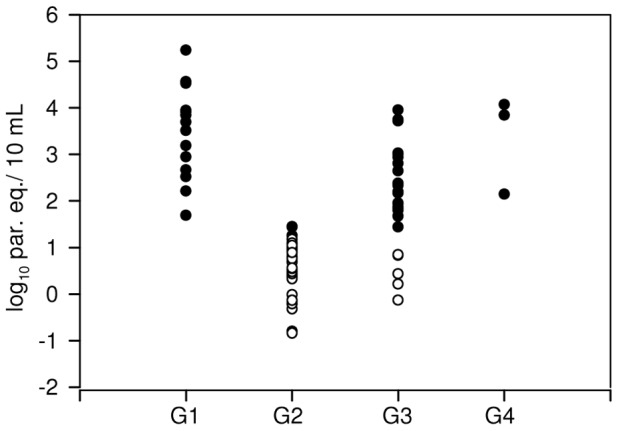
Methods/principal findings: We have standardized and validated a multiplex Real-Time quantitative PCR assay (qPCR) based on TaqMan technology, aiming to quantify T. cruzi satellite DNA as well as an internal amplification control (IAC) in a single-tube reaction. IAC amplification allows rule out false negative PCR results due to inhibitory substances or loss of DNA during sample processing. The assay has a limit of detection (LOD) of 0.70 parasite equivalents/mL and a limit of quantification (LOQ) of 1.53 parasite equivalents/mL starting from non-boiled Guanidine EDTA blood spiked with T. cruzi CL-Brener stock. The method was evaluated with blood samples collected from Chagas disease patients experiencing different clinical stages and epidemiological scenarios: 1- Sixteen Venezuelan patients from an outbreak of oral transmission, 2- Sixty three Bolivian patients suffering chronic Chagas disease, 3- Thirty four Argentinean cases with chronic Chagas disease, 4- Twenty seven newborns to seropositive mothers, 5- A seronegative receptor who got infected after transplantation with a cadaveric kidney explanted from an infected subject.
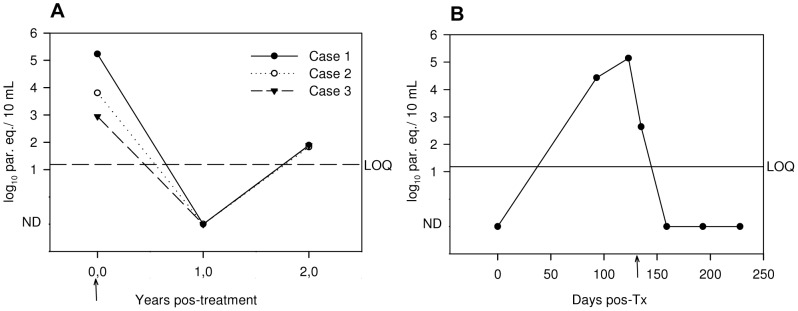
Conclusions/significance: The performing parameters of this assay encourage its application to early assessment of T. cruzi infection in cases in which serological methods are not informative, such as recent infections by oral contamination or congenital transmission or after transplantation with organs from seropositive donors, as well as for monitoring Chagas disease patients under etiological treatment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Special Programme for Research and Training in Tropical Disease (2007) Reporte del grupo de trabajo científico sobre la enfermedad de Chagas: 17–20 de abril de 2005, actualizado en julio de 2007, Buenos Aires, Argentina. Geneva: World Health Organization. 96 p.
-
- Feldman AM, Mac Namara D (2000) Myocarditis. N Engl J Med 343: 1388–1398. - PubMed
-
- Zingales B, Andrade SG, Briones MR, Campbell DA, Chiari E, et al. (2009) A new consensus for Trypanosoma cruzi intraspecific nomenclature: second revision meeting recommends TcI to TcVI. Mem Inst Oswaldo Cruz 104: 1051–1054. - PubMed
-
- Tibayrenc M (1998) Integrated genetic epidemiology of infectious diseases: the Chagas model. Mem Inst Oswaldo Cruz 93: 577–580. - PubMed
-
- Zingales B, Miles MA, Campbell DA, Tibayrenc M, Macedo AM, et al. (2012) The revised Trypanosoma cruzi subspecific nomenclature: rationale, epidemiological relevance and research applications. Infect Genet Evol 12: 240–253. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical