Phenotypic characterization of peripheral T cells and their dynamics in scrub typhus patients
- PMID: 22905277
- PMCID: PMC3419201
- DOI: 10.1371/journal.pntd.0001789
Phenotypic characterization of peripheral T cells and their dynamics in scrub typhus patients
Abstract
Background: Scrub typhus, caused by Orientia tsutsugamushi infection, is one of the main causes of febrile illness in the Asia-Pacific region. Although cell-mediated immunity plays an important role in protection, little is known about the phenotypic changes and dynamics of leukocytes in scrub typhus patients.
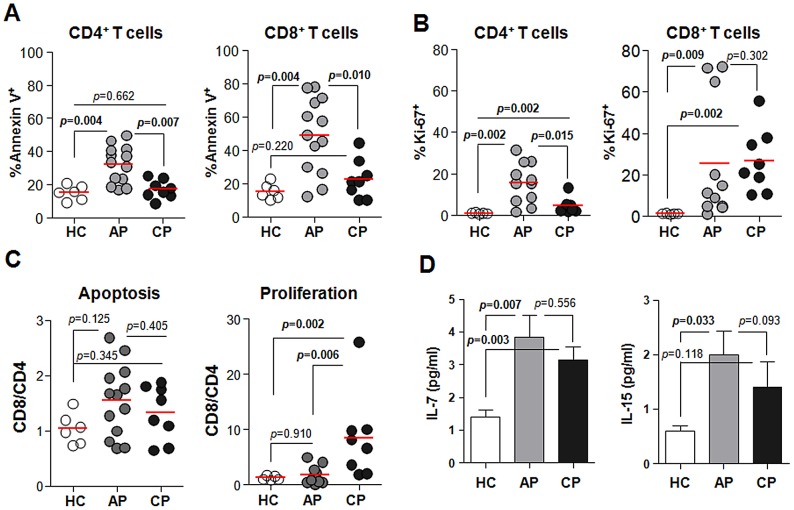
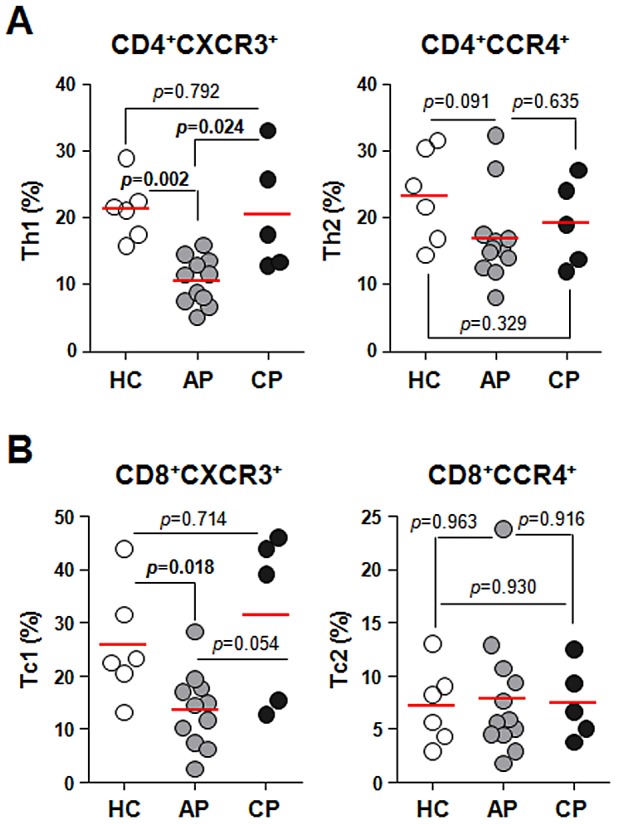
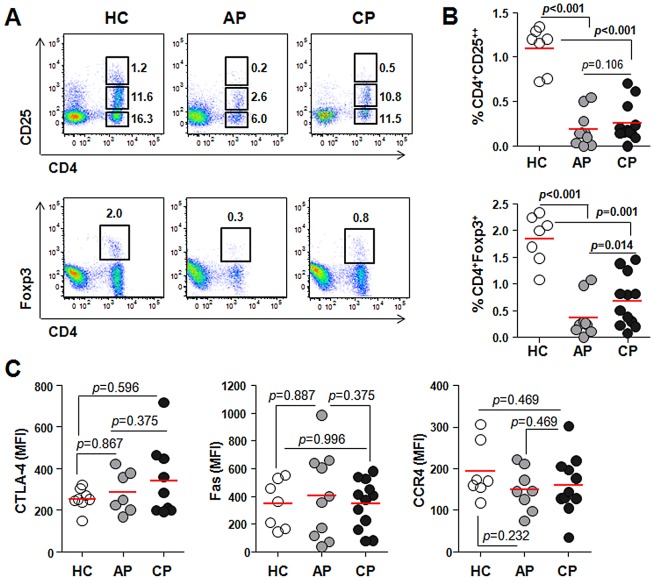
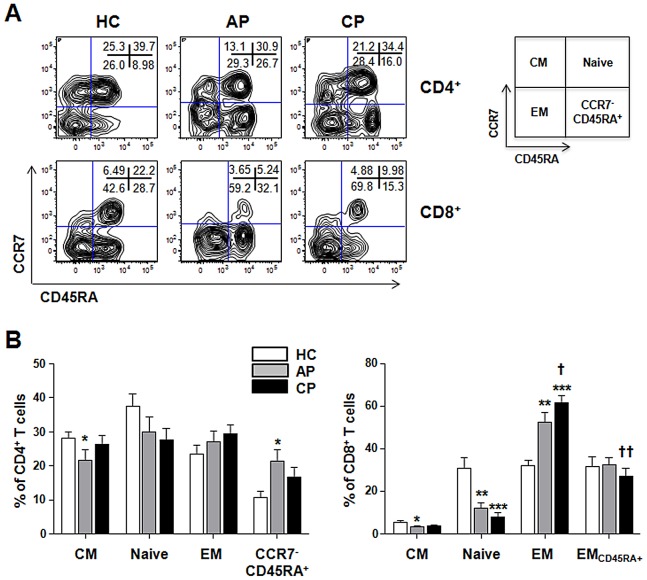
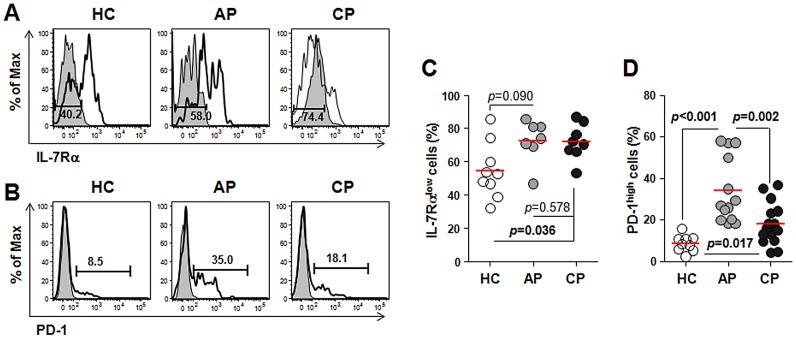
Methodology/principal findings: To reveal the underlying mechanisms of immunological pathogenesis, we extensively analyzed peripheral blood leukocytes, especially T cells, during acute and convalescent phases of infection in human patients and compared with healthy volunteers. We observed neutrophilia and CD4(+) T lymphopenia in the acute phase of infection, followed by proliferation of CD8(+) T cells during the convalescent phase. Massive T cell apoptosis was detected in the acute phase and preferential increase of CD8(+) T cells with activated phenotypes was observed in both acute and convalescent phases, which might be associated or correlated with elevated serum IL-7 and IL-15. Interestingly, peripheral Treg cells were significantly down-regulated throughout the disease course.
Conclusions/significance: The remarkable decrease of CD4(+) T cells, including Treg cells, during the acute phase of infection may contribute to the loss of immunological memory that are often observed in vaccine studies and recurrent human infection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Seong SY, Choi MS, Kim IS (2001) Orientia tsutsugamushi infection: overview and immune responses. Microbes Infect 3: 11–21. - PubMed
-
- Richards AL (2004) Rickettsial vaccines: the old and the new. Expert Rev Vaccines 3: 541–555. - PubMed
-
- Mathai E, Rolain JM, Verghese GM, Abraham OC, Mathai D, et al. (2003) Outbreak of scrub typhus in southern India during the cooler months. Ann N Y Acad Sci 990: 359–364. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials