Refining the global spatial limits of dengue virus transmission by evidence-based consensus
- PMID: 22880140
- PMCID: PMC3413714
- DOI: 10.1371/journal.pntd.0001760
Refining the global spatial limits of dengue virus transmission by evidence-based consensus
Abstract
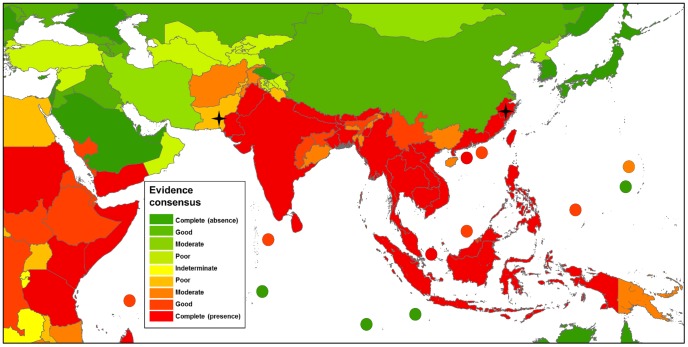
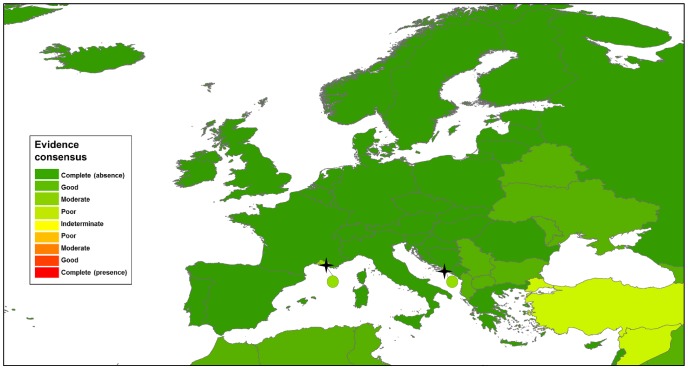
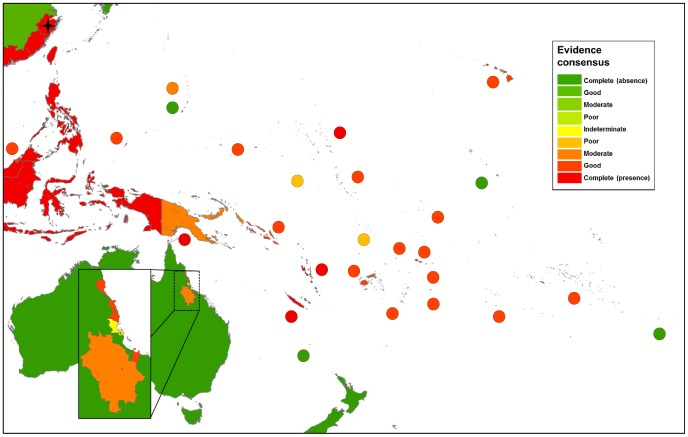
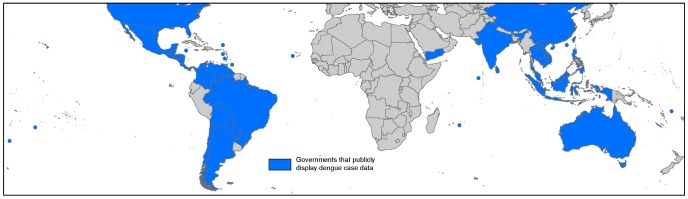
Background: Dengue is a growing problem both in its geographical spread and in its intensity, and yet current global distribution remains highly uncertain. Challenges in diagnosis and diagnostic methods as well as highly variable national health systems mean no single data source can reliably estimate the distribution of this disease. As such, there is a lack of agreement on national dengue status among international health organisations. Here we bring together all available information on dengue occurrence using a novel approach to produce an evidence consensus map of the disease range that highlights nations with an uncertain dengue status.
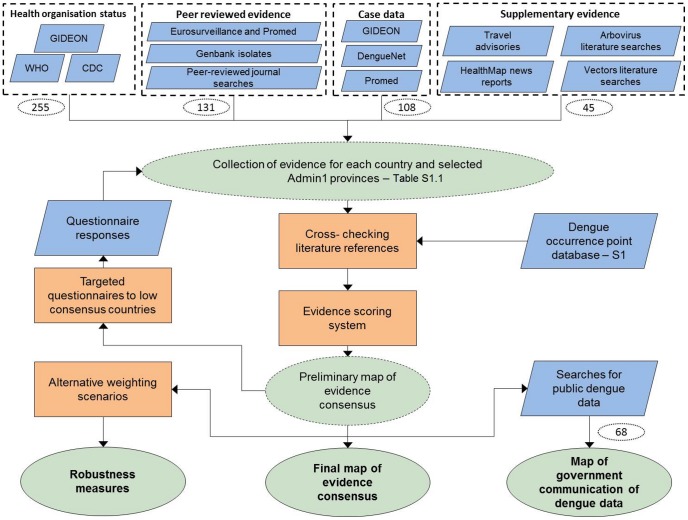
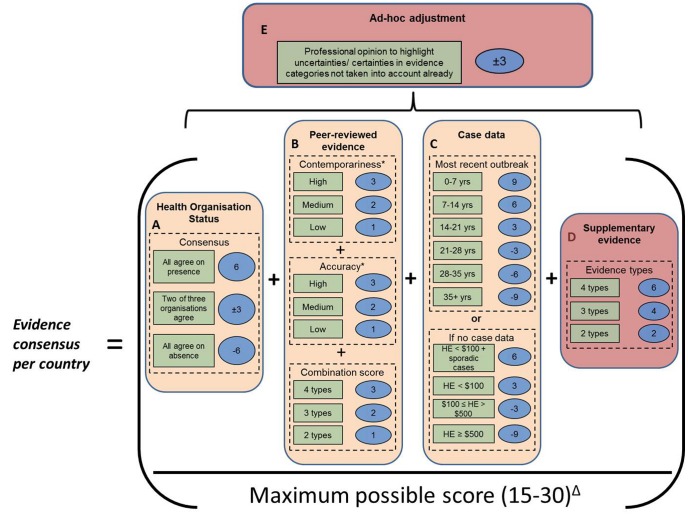
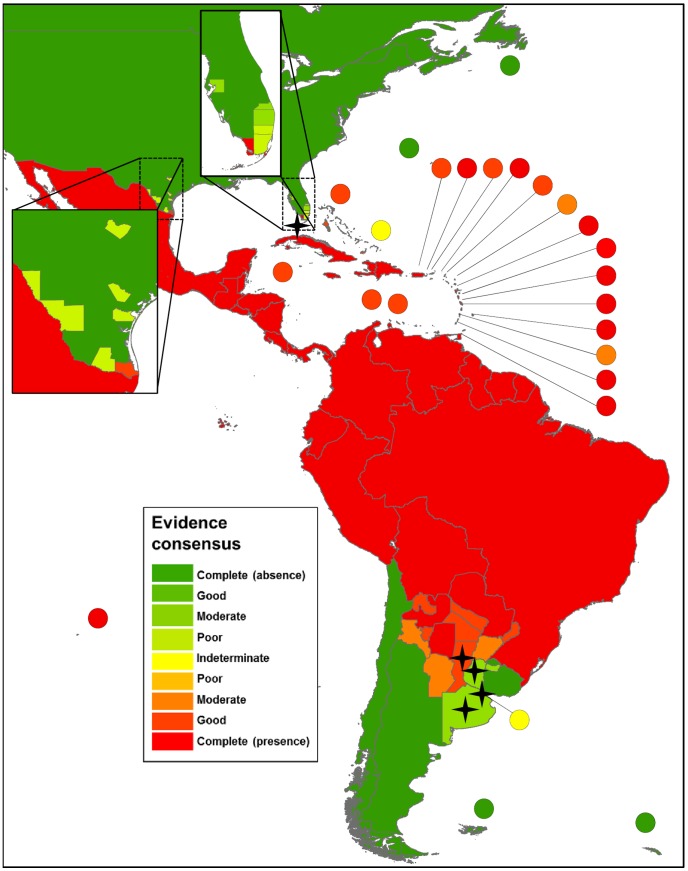
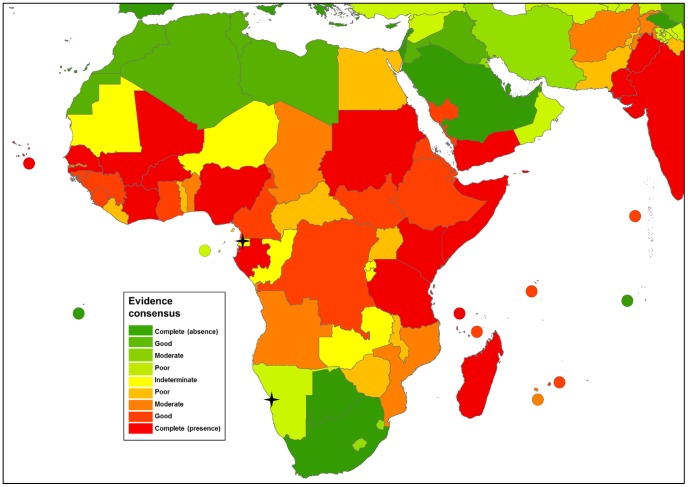
Methods/principal findings: A baseline methodology was used to assess a range of evidence for each country. In regions where dengue status was uncertain, additional evidence types were included to either clarify dengue status or confirm that it is unknown at this time. An algorithm was developed that assesses evidence quality and consistency, giving each country an evidence consensus score. Using this approach, we were able to generate a contemporary global map of national-level dengue status that assigns a relative measure of certainty and identifies gaps in the available evidence.
Conclusion: The map produced here provides a list of 128 countries for which there is good evidence of dengue occurrence, including 36 countries that have previously been classified as dengue-free by the World Health Organization and/or the US Centers for Disease Control. It also identifies disease surveillance needs, which we list in full. The disease extents and limits determined here using evidence consensus, marks the beginning of a five-year study to advance the mapping of dengue virus transmission and disease risk. Completion of this first step has allowed us to produce a preliminary estimate of population at risk with an upper bound of 3.97 billion people. This figure will be refined in future work.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Hales S, de Wet N, Maindonald J, Woodward A (2002) Potential effect of population and climate changes on global distribution of dengue fever: an empirical model. Lancet 360: 830–834. - PubMed
-
- Beatty M, Letson W, Edgil D, Margolis H (2007) Estimating the total world population at risk for locally acquired dengue infection. Philadelphia. 170–257.
-
- WHO (2009) Dengue guidelines for diagnosis, treatment, prevention and control. In: Ciceri K, Tissot P, editors. 2009 ed. Geneva: World Health Organization. - PubMed
-
- Tapia-Conyer R, Mendez-Galvan JF, Gallardo-Rincon H (2009) The growing burden of dengue in Latin America. Journal of clinical virology : the official publication of the Pan American Society for Clinical Virology 46 Suppl 2: S3–6. - PubMed
-
- Van Kleef E, Bambrick H, Hales S (2010) The geographic distribution of dengue fever and the potential influence of global climate change. TropIKA 1–18.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials