Epidemiological and entomological evaluations after six years or more of mass drug administration for lymphatic filariasis elimination in Nigeria
- PMID: 22022627
- PMCID: PMC3191131
- DOI: 10.1371/journal.pntd.0001346
Epidemiological and entomological evaluations after six years or more of mass drug administration for lymphatic filariasis elimination in Nigeria
Abstract
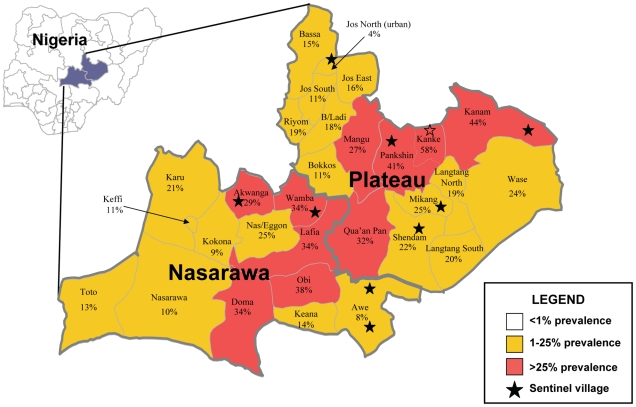
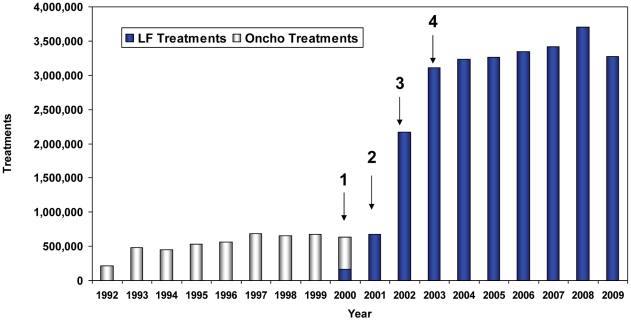
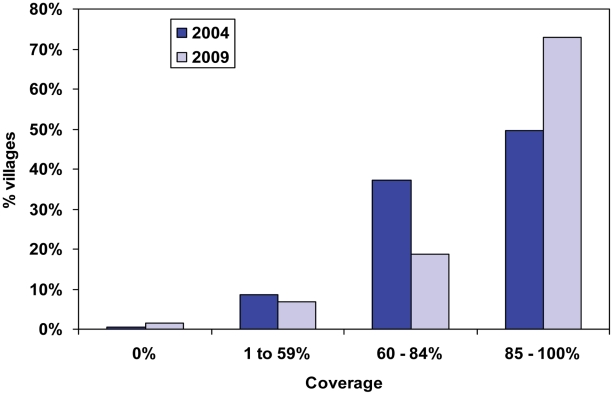
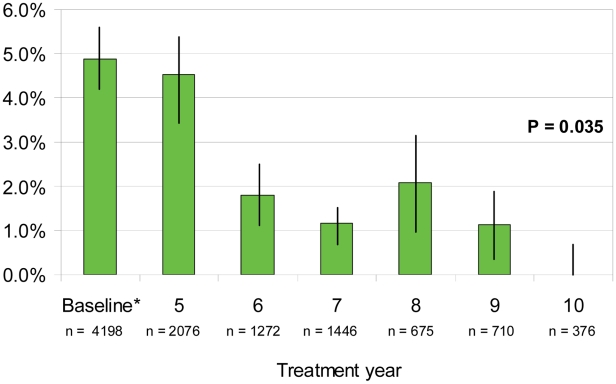
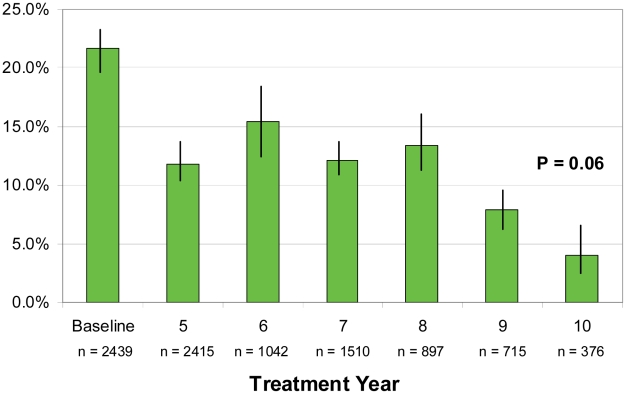
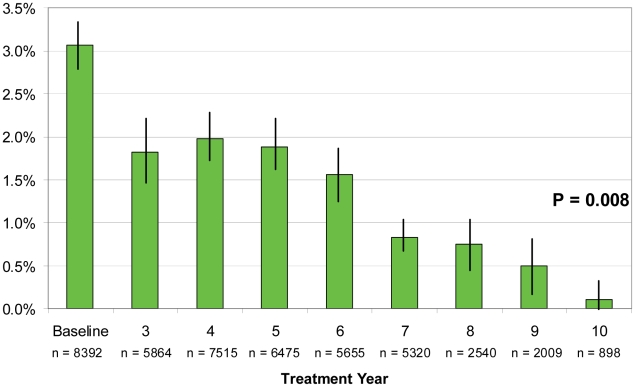
The current strategy for interrupting transmission of lymphatic filariasis (LF) is annual mass drug administration (MDA), at good coverage, for 6 or more years. We describe our programmatic experience delivering the MDA combination of ivermectin and albendazole in Plateau and Nasarawa states in central Nigeria, where LF is caused by anopheline transmitted Wuchereria bancrofti. Baseline LF mapping using rapid blood antigen detection tests showed mean local government area (LGA) prevalence of 23% (range 4-62%). MDA was launched in 2000 and by 2003 had been scaled up to full geographic coverage in all 30 LGAs in the two states; over 26 million cumulative directly observed treatments were provided by community drug distributors over the intervention period. Reported treatment coverage for each round was ≥85% of the treatment eligible population of 3.7 million, although a population-based coverage survey in 2003 showed lower coverage (72.2%; 95% CI 65.5-79.0%). To determine impact on transmission, we monitored three LF infection parameters (microfilaremia, antigenemia, and mosquito infection) in 10 sentinel villages (SVs) serially. The last monitoring was done in 2009, when SVs had been treated for 7-10 years. Microfilaremia in 2009 decreased by 83% from baseline (from 4.9% to 0.8%); antigenemia by 67% (from 21.6% to 7.2%); mosquito infection rate (all larval stages) by 86% (from 3.1% to 0.4%); and mosquito infectivity rate (L3 stages) by 76% (from 1.3% to 0.3%). All changes were statistically significant. Results suggest that LF transmission has been interrupted in 5 of the 10 SVs, based on 2009 finding of microfilaremia ≥1% and/or L3 stages in mosquitoes. Four of the five SVs where transmission persists had baseline antigenemia prevalence of >25%. Longer or additional interventions (e.g., more frequent MDA treatments, insecticidal bed nets) should be considered for 'hot spots' where transmission is ongoing.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Lymphatic filariasis. Fourth report of the WHO Expert Committee on Filariasis. World Health Organ Tech Rep Ser. 1984;702:3–112. - PubMed
-
- Preventative chemotherapy in human helminthiasis. 2006. Coordinated use of anthelminthic drugs in control interventions: a manual for health professionals and programme managers. World Health Organization.
-
- Guidelines for certifying lymphatic filariasis elimination (including discussion of critical issues and rationale). 1999. World Health Organization.
-
- Molyneux DH, Zagaria N. Lymphatic filariasis elimination: progress in global programme development. Ann Trop Med Parasitol. 2002;96(Suppl 2):S15–40. - PubMed
-
- Ottesen EA. Lymphatic filariasis: Treatment, control and elimination. Adv Parasitol. 2006;61:395–441. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources