Efficacy of praziquantel and artemisinin derivatives for the treatment and prevention of human schistosomiasis: a systematic review and meta-analysis
- PMID: 22004571
- PMCID: PMC3207908
- DOI: 10.1186/1756-3305年4月20日1
Efficacy of praziquantel and artemisinin derivatives for the treatment and prevention of human schistosomiasis: a systematic review and meta-analysis
Abstract
Background: Praziquantel has been used as first-line drug for chemotherapy of schistosomiasis since 1984. Besides praziquantel, artemether and artesunate have also been used for the control of this infectious disease since late 1990s. In this article, we conducted a systematic review and meta-analysis to evaluate the antischistosomal efficacy of different medication strategies including monotherapy or combination therapies of these drugs.
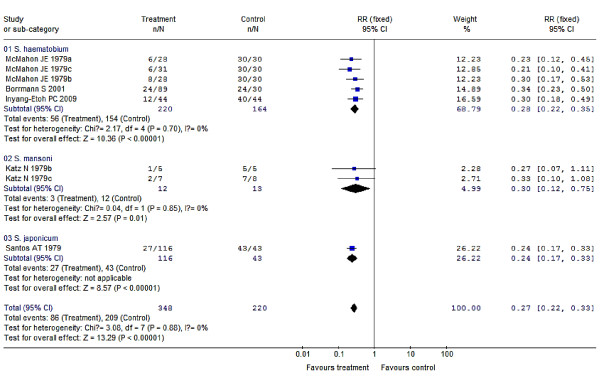
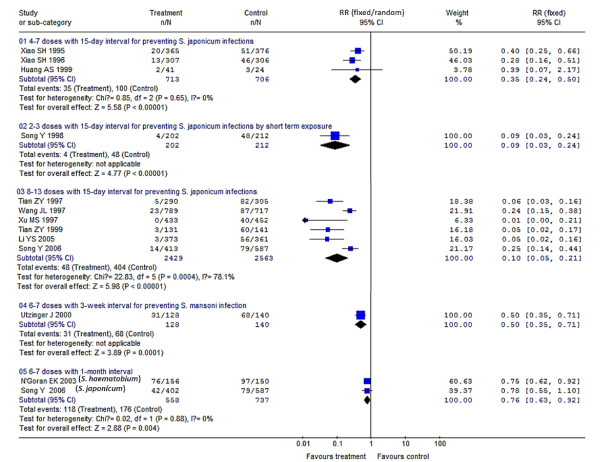
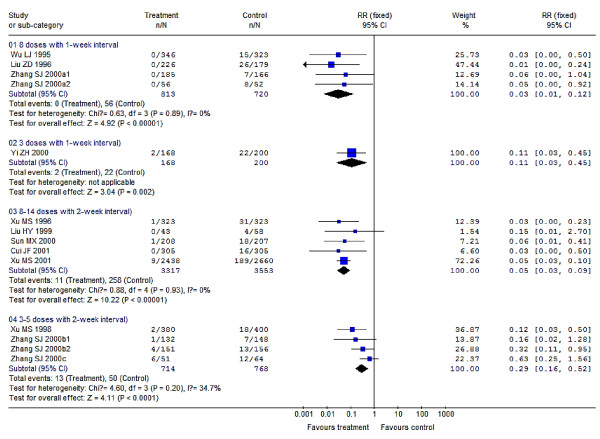
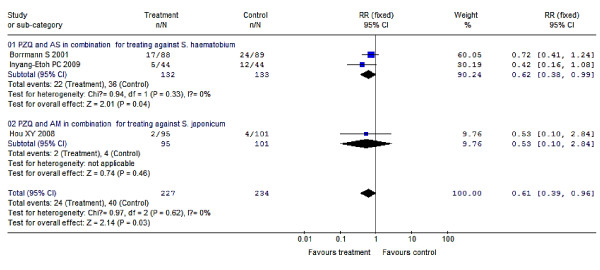
Results: A number of 52 trials from 38 articles published in peer-reviewed journals before July 2011 were selected for analysis after searching the following literature databases: the Cochrane Library, PubMed/Medline, ISI Web of Science, Chinese Biomedicine Literature Database, and China National Knowledge Infrastructure. Our meta-analyses showed that a dosage of 30-60 mg/kg praziquantel compared with placebo produced a protection rate of about 76% (95% CI: 67%-83%) for treating human schistosomiasis, which varied from 70% to 76% with no significant differences among the subspecies S. haematobium, S. japonicum or S. mansoni. Protection rates were higher when praziquantel doses were elevated, as concluded from the nRCTs results: the protection rate of praziquantel at 40 mg/kg was 52% (95% CI: 49%-55%), and it increased to 91% (95% CI: 88%-92%) when the dosages were elevated to 60/80/100 mg/kg divided two or more doses. Multiple doses of artemether or artesunate over 1- or 2-week intervals resulted in protection rates of 65% to 97% for preventing schistosomiasis, and increased doses and shorter medication intervals improved their efficacies. Praziquantel and artemisinin derivatives (artemether or artesunate) in combination resulted in a higher protection rate of 84% (95% CI: 64%-91%) than praziquantel monotherapy for treatment. praziquantel and artesunate in combination had a great protection rate of 96% (95% CI: 78%-99%) for preventing schistosomes infection.
Conclusions: According to the results, praziquantel remains effective in schistosomiasis treatment, and multiple doses would improve its efficacy; meanwhile, praziquantel is also a good drug for preventing acute schistosomiasis morbidity. It's better to use multiple doses of artemether or artesunate with 1- or 2-week intervals for prevention against schistosome infection. Praziquantel and artemether or artesunate in combination perform better in treatment than praziquantel monotherapy, and they are especially suitable for treating the patients with repeated exposure to infected water.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases