Retracing micro-epidemics of Chagas disease using epicenter regression
- PMID: 21935346
- PMCID: PMC3174153
- DOI: 10.1371/journal.pcbi.1002146
Retracing micro-epidemics of Chagas disease using epicenter regression
Abstract
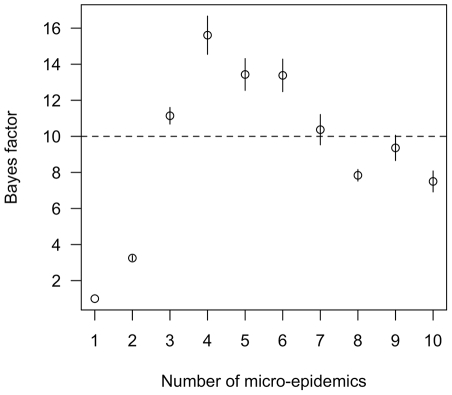
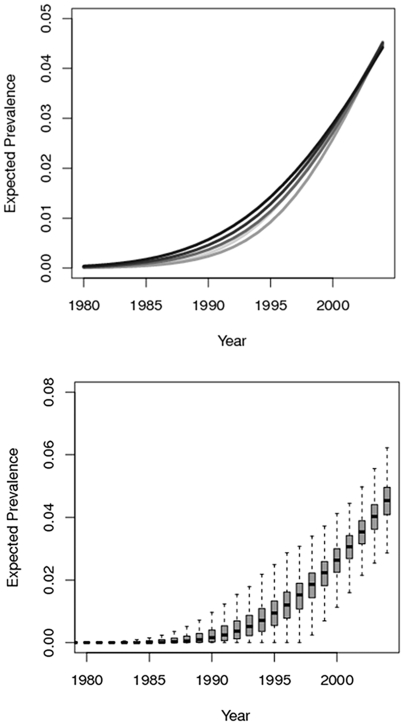
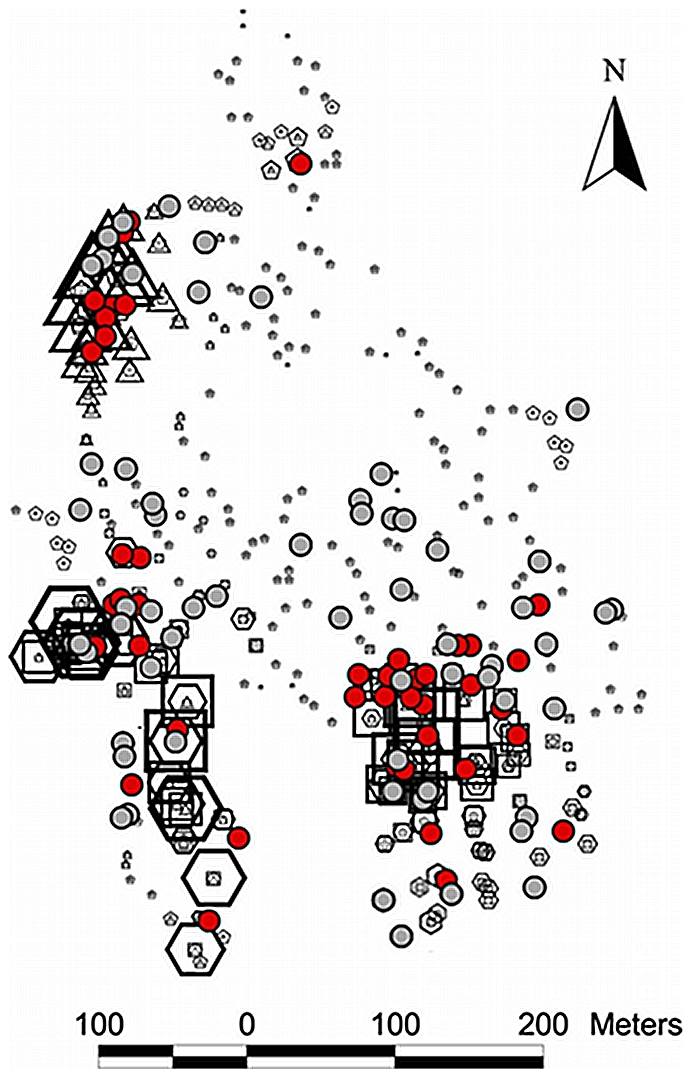
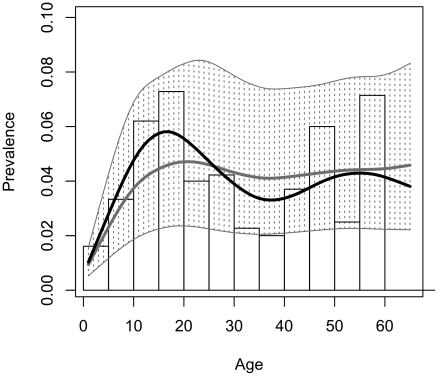
Vector-borne transmission of Chagas disease has become an urban problem in the city of Arequipa, Peru, yet the debilitating symptoms that can occur in the chronic stage of the disease are rarely seen in hospitals in the city. The lack of obvious clinical disease in Arequipa has led to speculation that the local strain of the etiologic agent, Trypanosoma cruzi, has low chronic pathogenicity. The long asymptomatic period of Chagas disease leads us to an alternative hypothesis for the absence of clinical cases in Arequipa: transmission in the city may be so recent that most infected individuals have yet to progress to late stage disease. Here we describe a new method, epicenter regression, that allows us to infer the spatial and temporal history of disease transmission from a snapshot of a population's infection status. We show that in a community of Arequipa, transmission of T. cruzi by the insect vector Triatoma infestans occurred as a series of focal micro-epidemics, the oldest of which began only around 20 years ago. These micro-epidemics infected nearly 5% of the community before transmission of the parasite was disrupted through insecticide application in 2004. Most extant human infections in our study community arose over a brief period of time immediately prior to vector control. According to our findings, the symptoms of chronic Chagas disease are expected to be absent, even if the strain is pathogenic in the chronic phase of disease, given the long asymptomatic period of the disease and short history of intense transmission. Traducción al español disponible en Alternative Language Text S1/A Spanish translation of this article is available in Alternative Language Text S1.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- WHO Expert Committee. Control of Chagas Disease. 109; WHO Technical Report Series Number. 2002;905:1. - PubMed
-
- Bowman NM, Kawai V, Levy MZ, Cornejo del Carpio JG, Cabrera L, et al. Chagas disease transmission in periurban communities of Arequipa, Peru. Clin Infect Dis. 2008;46:1822–8. - PubMed
-
- Fraser B. Controlling Chagas' disease in urban Peru. Lancet. 2008;372:16–7. - PubMed
-
- Magalhaes JB, Pontes AL, Andrade SG. Behavior of the Y and Peruvian strains of trypanosoma cruzi in mice, after passage through various media. Mem Inst Oswaldo Cruz. 1985;80:41–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials