Integrated monitoring and evaluation and environmental risk factors for urogenital schistosomiasis and active trachoma in Burkina Faso before preventative chemotherapy using sentinel sites
- PMID: 21749703
- PMCID: PMC3161883
- DOI: 10.1186/1471-2334年11月19日1
Integrated monitoring and evaluation and environmental risk factors for urogenital schistosomiasis and active trachoma in Burkina Faso before preventative chemotherapy using sentinel sites
Abstract
Background: Over 1 billion of the world's poorest inhabitants are afflicted by neglected tropical diseases (NTDs). Integrated control programmes aimed at tackling these debilitating NTDs have been recently initiated, mainly using preventative chemotherapy. Monitoring and evaluation (M&E) of these integrated programs presents particular challenges over and above those required for single disease vertical programmes. We used baseline data from the National NTD Control Programme in Burkina Faso in order to assess the feasibility of an integrated survey design, as well as to elucidate the contribution of environmental variables to the risk of either Schistosoma haematobium, trachoma, or both among school-aged children.
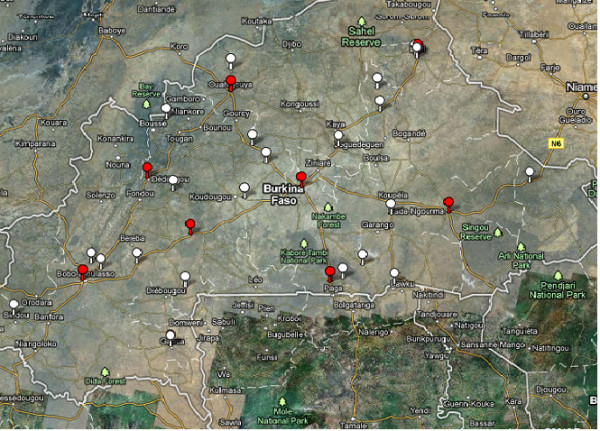
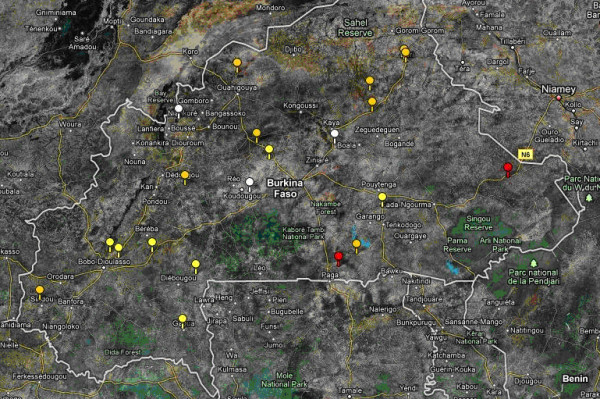
Methods: S. haematobium infection was diagnosed by detecting eggs in urine. A trachoma case was defined by the presence of Trachomatous inflammation-Follicular (TF) and/or Trachomatous inflammation-Intense (TI) in either eye. Baseline data collected from 3,324 children aged 7-11 years in 21 sentinel sites across 11 regions of Burkina Faso were analyzed using simple and multivariable hierarchical binomial logistic regression models fitted by Markov Chain Monte Carlo estimation methods. Probabilities of the risk of belonging to each infection/disease category were estimated as a function of age, gender (individual level), and environmental variables (at sentinel site level, interpolated from national meteorological stations).
Results: Overall prevalence at the sentinel sites was 11.79% (95% CI: 10.70-12.89) for S. haematobium; 13.30% (12.14-14.45) for trachoma and 0.84% (0.53-1.15) for co-infections. The only significant predictor of S. haematobium infection was altitude. There were significant negative associations between the prevalence of active trachoma signs and minimum temperature, and air pressure. Conditional upon these predictors, these data are consistent with the two pathogens being independent.
Conclusions: Urogenital schistosomiasis and trachoma constitute public health problems in Burkina Faso. Sentinel site (at school level) surveys for these two NTDs can be implemented simultaneously. However, to support MDA treatment decisions in Burkina Faso, the protocol used in this study would only be applicable to hypoendemic trachoma areas. More research is needed to confirm if these findings can be generalized to West Africa and beyond.
Figures
{kind=link}
{kind=link}
References
-
- Fenwick A, Molyneux D, Nantulya V. Achieving the Millennium Development Goals. Lancet. 2005;365(9464):1029–1030. - PubMed
-
- WHO. Social and Economic Research Reports TAR/SER/PRS. Geneva: WHO; 1995. Identification of high-risk communities for control of schistosomiasis in Africa: A multicommunity study; p. 83.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous