Vaccines to combat the neglected tropical diseases
- PMID: 21198676
- PMCID: PMC3438653
- DOI: 10.1111/j.1600-065X.2010.00976.x
Vaccines to combat the neglected tropical diseases
Abstract
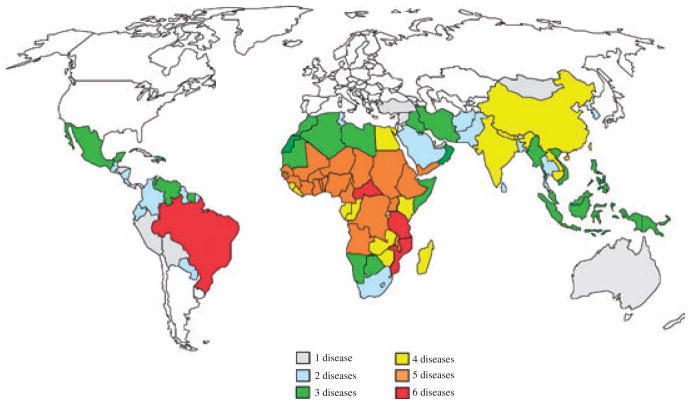
The neglected tropical diseases (NTDs) represent a group of parasitic and related infectious diseases such as amebiasis, Chagas disease, cysticercosis, echinococcosis, hookworm, leishmaniasis, and schistosomiasis. Together, these conditions are considered the most common infections in low- and middle-income countries, where they produce a level of global disability and human suffering equivalent to better known conditions such as human immunodeficiency virus/acquired immunodeficiency syndrome and malaria. Despite their global public health importance, progress on developing vaccines for NTD pathogens has lagged because of some key technical hurdles and the fact that these infections occur almost exclusively in the world's poorest people living below the World Bank poverty line. In the absence of financial incentives for new products, the multinational pharmaceutical companies have not embarked on substantive research and development programs for the neglected tropical disease vaccines. Here, we review the current status of scientific and technical progress in the development of new neglected tropical disease vaccines, highlighting the successes that have been achieved (cysticercosis and echinococcosis) and identifying the challenges and opportunities for development of new vaccines for NTDs. Also highlighted are the contributions being made by non-profit product development partnerships that are working to overcome some of the economic challenges in vaccine manufacture, clinical testing, and global access.
© 2010 John Wiley & Sons A/S.
Figures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
-
- Hotez P. Forgotten People, Forgotten Diseases: The Neglected Tropical Diseases and their Impact on Global Health and Development. Washington, DC: American Society for Microbiology Press; 2008.
-
- Collier P. The Bottom Billion: Why the Poorest Countries Are Failing and What Can Be Done About It. Oxford: Oxford University Press; 2007.
-
- Hotez PJ, Ferris MT. The antipoverty vaccines. Vaccine. 2006;24:5787–5799. - PubMed
-
- Hotez P. Combating parasitic diseases in innovative developing countries by reverse vaccinology. Parasite Immunol. 2006;28:242–243.
-
- Hotez PJ. A plan to defeat neglected tropical diseases. Sci Am. 2010;302:90–94. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical